4.4.2. Bàn luận về nhiễm khuẩn ối
Có thể thấy rõ mối liên hệ giữa sự xâm nhập của vi khuẩn đường sinh dục và ối vỡ non. Nhiều loại vi sinh vật xâm nhập vào đường sinh dục dưới có khả năng sản xuất phospholipases, kích thích sự sản xuất prostaglandin và do đó dẫn đến sự khởi phát của cơn co tử cung. Ngoài ra, phản ứng miễn dịch của bệnh nhân do sự xâm nhập của vi khuẩn ở âm đạo, cổ tử cung và màng ối dẫn đến việc sản xuất ra nhiều chất trung gian hóa học của phản ứng viêm, có thể làm giảm sự bền vững của màng ối và kết quả gây ra nước ối trên thai non tháng. Sau khi có hiện tượng ra nước ối, tức là có sự thông thương giữa buồng ối và môi trường bên ngoài, đặc biệt là môi trường âm đạo có các vi khuẩn, sẽ xâm nhập vào buồng ối dẫn đến hiện tượng nhiễm trùng ối.
Nghiên cứu của chúng tôi cho tỷ lệ nghi ngờ nhiễm trùng ối là 16,44%. Tỷ lệ này thấp hơn so với trong nghiên cứu của Lê Thu Thuỷ là 18,9% [54] và nghiên cứu của Yu H ở Trung Quốc là 17,8% [32].
4.4.3. Nhận xét tình trạng trẻ sơ sinh
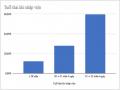
Theo bảng 3.17, cân nặng trung bình của trẻ sinh ra ở sản phụ có ối vỡ non trung bình là 1808 ± 449 gr, trẻ nhẹ cân nhất là 900 gr, nặng cân nhất là 2500 gr. Kết quả của chúng tôi tương tự như nghiên cứu của Yu trên 510 trường hợp sản phụ có OVN tuổi thai dưới 34 tuần, sinh con với cân nặng trung bình là 1815,1 ± 462,6g [32]. Nghiên cứu của Nicaise trên 118 trường hợp ra nước ối ở thai 24 – 34 tuần cho kết quả cân nặng thấp nhất là 600g, cao nhất là 3260g, cân nặng trung bình là 1487 ± 490g [72].
Sơ sinh cân nặng thấp là một trong những hậu quả của việc sinh non sau khi ối vỡ vì những trẻ này đều sinh khi chưa đủ tháng, cân nặng thấp, ngoài ra còn sẽ kèm theo các biến chứng khác kèm theo do thai non tháng, dẫn đến nuôi dưỡng khó khăn và tốn kém, chưa kể đến những biến chứng lâu dài về sau.
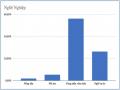
Theo bảng 3.17, Chỉ số Apgar 1 phút, có 30,14% bé bị ngạt (<7), số bé không bị ngạt chiếm 69,86%. Chỉ số Apgar 5 phút, hầu hết các bé không ngạt chiếm 79,45%,
còn lại là số bé bị ngạt chiếm 20,55%. Y văn đã chứng minh việc kéo dài thêm tuổi thai trong ối vỡ non đã giúp cải thiện đáng kể tỷ lệ ngạt sơ sinh.
4.4.4. Nhận xét về bệnh lý của trẻ sơ sinh
Trong nghiên cứu của chúng tối, chỉ tập trung vào những biến chứng gần: tỷ lệ suy hô hấp sơ sinh là 49,32%, tỷ lệ nhiễm khuẩn sơ sinh là 41,09%.
Theo bảng 3.19, số trẻ bị nhiễm khuẩn sơ sinh là 41,09%, trong đó có 1 trẻ bị biến chứng viêm ruột hoại tử. Theo tác giá Võ Minh Tuấn và cộng sự nghiên cứu ở 689 trường hợp ối vỡ non ở tuổi thai từ 28 – 34 tuần tại bệnh viện Từ Dũ năm 2007
- 2008, tỷ lệ này là 54,39% [73]. Tỷ lệ nhiễm khuẩn sơ sinh trong nghiên cứu của chúng tôi thấp hơn chủ yếu do những tiến bộ trong điều trị đối với những trẻ sơ sinh non tháng.
Tỷ lệ trẻ suy hô hấp sau sinh chiếm tỷ lệ thấp hơn trẻ không có suy hô hấp, lần lượt là 49,32% và 50,68%. Theo tác giá Võ Minh Tuấn và cộng sự nghiên cứu ở 689 trường hợp ối vỡ non ở tuổi thai từ 28 – 34 tuần tại bệnh viện Từ Dũ năm 2007 - 2008, tỷ lệ này là 49,56% [73].
KẾT LUẬN
Từ những kết quả nghiên cứu trên 73 trường hợp sản phụ được chẩn đoán OVN, chúng tôi rút ra được một số kết luận sau:
1. Một số đặc điểm lâm sàng, cận lâm sàng
- Trong số các sản phụ OVN có 11% sản phụ có tiền sử đẻ non trước đó.
- Có 13,7% các sản phụ có thai nhờ thụ tinh trong ống nghiệm.
- 57,53% các sản phụ có tình trạng nước ối giảm từ khi nhập viện.
- Tỷ lệ các sản phụ OVN có tăng CRP khi nhập viện rất thấp, chiếm 4,11%.
- Tuổi thai khi nhập viện trung bình là 31,63 ± 2,27 tuần, tuổi thai nhỏ nhất là 24 tuần 3 ngày, lớn nhất là 33 tuần 6 ngày tuổi.
2. Kết quả điều trị
- Có 82,19% sản phụ kéo dài thêm được tuổi thai. Tuổi thai kéo dài thêm trung bình là 12,11 ± 5,39 ngày. Thời gian kéo dài thêm lâu nhất là 48 ngày.
- 56,16% các tường hợp chỉ phải sử dụng 01 loại kháng sinh dự phòng trong vòng 7-10 ngày.
- 98,63% các trường hợp sử dụng được ít nhất 01 mũi trưởng thành phổi trước khi sinh.
- Tỷ lệ nhiễm khuẩn ối là 16,44%.
- 63,01% các sản phụ OVN đã đẻ đường âm đạo.
- OVN có kèm theo vết mổ cũ là lý do lớn nhất dẫn tới chỉ định mổ lấy thai chiếm 37,04%.
- Trẻ sơ sinh có cân nặng trung bình 1808g ± 449g.
- Có 49,36% các trường hợp trẻ sơ sinh có suy hô hấp.
- Tỷ lệ nhiễm khuẩn sơ sinh là 41,09%.
TÀI LIỆU THAM KHẢO
BM. Mercer, “"Preterm premature rupture of the membranes: current approaches to evaluation and management", Obstetrics and Gynecology Clinics of North America,” pp. 411-428, 2005. | |
[2] | BM. Mercer, “"Preterm premature rupture of the membranes", Obstetrics and Gynecology, 101, pp. 178-193.,” pp. 178-193, 2003. |
[3] | Jean-Charles Pasquier; Muriel Rabilloud ; Jean-Charles Picaud; Rene ́ Ecochard; Olivier Claris; Pascal Gaucherand ;Fre ́de ́ric Collet; Pierre Chabert; Georges Mellier., “A prospective population-based study of 598 cases of PPROM between 24 and 34 weeks’ gestation: description, management, and mortality (DOMINOS cohort),” 2004. |
[4] | MJ Keirse, A Ohission, PE Treffers et al, “"Prelabour rupture of the membranes preterm", Effective care in pregnancy and chidbirth, Oxford University Press, Oxford,” p. 666, 1989. |
[5] | Williams Obstetrics, Williams Obstetrics 25th, 2018, p. 1970 – 1972. |
[6] | Michael Tchirikov*, Natalia Schlabritz-Loutsevitch, James Maher, Jörg Buchmann, Yuri Naberezhnev, Andreas S. Winarno and Gregor Seliger, “Mid-trimester preterm premature rupture of membranes (PPROM): etiology, diagnosis, classification, international recommendations of treatment options and outcome,” 2017. |
[7] | B. Mercer, “"Premature Rupture of the Membranes", Obstetrics - Normal and problem pregnancies, Elsevier,” p. 713, 2007. |
[8] | J. H. Harger, A. W. Hsing, R. E. Tuomala et al, “"Risk factors for preterm premature rupture of fetal membranes: a multicenter case- control study", American Journal of Obstetrics and Gynecology,” pp. 130-137, 1990. |
[9] | E. Lorthe a,*,b, “Epidemiology, risk factors and child prognosis: CNGOF Preterm Premature Rupture of Membranes Guidelines,” 2018. |
[10] | B. M. Mercer, R. L. Goldenberg, A. H. Moawad et al, “"The preterm prediction study: effect of gestational age and cause of preterm birth on subsequent obstetric outcome. National Institute of Child Health and Human Development Maternal-Fetal Medicine Units Network", American Journal of Obstetrics and Gyneco,” pp. 1216- 1221, 1999. |
[11] | Thomas Lee, Marshall W. Carpenter, Walter W. Heber et al, “Preterm premature rupture of membranes: risks of recurrent complications in the next pregnancy among a population-based sample of gravid women", American Journal of Obstetrics and Gynecology,” pp. 209-213, 2003. |
[12] | J. H. Harger, A. W. Hsing, R. E. Tuomala et al, “"Risk factors for preterm premature rupture of fetal membranes: a multicenter case- control study", American Journal of Obstetrics and Gynecology,” pp. 130-137, 1990. |
[13] | K. M. Davidson, “"Detection of premature rupture of the membranes",” Clinical Obstetrics and Gynecology, pp. 715-722, 1991. |
[14] | Kunze M, Klar M, Morfeld CA, Thorns B, Schild RL, Markfeld-Erol F, et al., “Cytokines in noninvasively obtained amniotic fluid as predictors of fetal inflammatory response syndrome. Am J Obstet Gynecol. 2016;215:96,” 2016. |
Có thể bạn quan tâm!
-
 Đặc Điểm Lâm Sàng Và Cận Lâm Sàng Của Đối Tượng Nghiên Cứu.
Đặc Điểm Lâm Sàng Và Cận Lâm Sàng Của Đối Tượng Nghiên Cứu. -
 Phân Bố Tuổi Thai Khi Nhập Viện Của Sản Phụ Có Ovn
Phân Bố Tuổi Thai Khi Nhập Viện Của Sản Phụ Có Ovn -
 Phân Bố Ối Vỡ Non Theo Đặc Điểm Tình Trạng Nước Ối
Phân Bố Ối Vỡ Non Theo Đặc Điểm Tình Trạng Nước Ối -
 Nhận xét kết quả điều trị ối vỡ non tuổi thai từ 24 tuần 0 ngày đến 33 tuần 6 ngày tại Bệnh viện phụ sản Hà Nội trong 6 tháng cuối năm 2021 - 10
Nhận xét kết quả điều trị ối vỡ non tuổi thai từ 24 tuần 0 ngày đến 33 tuần 6 ngày tại Bệnh viện phụ sản Hà Nội trong 6 tháng cuối năm 2021 - 10
Xem toàn bộ 84 trang tài liệu này.
Adekola H, Gill N, Sakr S, Hobson D, Bryant D, Abramowicz JS, et al., “Outcomes following intra-amniotic instillation with indigo carmine to diagnose prelabor rupture of membranes in singleton pregnancies: a single center experience. J Matern Fetal Neonatal”. | |
[16] | Beckmann MW, Wiegratz I, Dereser MM, Baier P, Born HJ. Diag- nostik des Blasensprungs, “Diag- nostik des Blasensprungs: Vergleich des vaginalen Nachweises von fetalem Fibronectin und der intraamnialen Injektion von Indigo Carmine. Geburtshilfe Frauenheilk. 1993;53:86–91.,” 1993. |
[17] | Sosa CG, Herrera E, Restrepo JC, Strauss A, Alonso J., “Compari- son of placental alpha microglobulin-1 in vaginal fluid with intra-amniotic injection of indigo carmine for the diagnosis of rupture of membranes. J Perinat Med. 2014;42:611–6.,” 2014. |
[18] | London: National Institute for Health and Care Excellence (NICE), “Preterm labour and birth,” 2019. |
[19] | FIGO Working Group on Good Clinical Practice in Maternal–Fetal Medicine, “Good clinical practice advice: Prediction of preterm labor and preterm premature rupture of membranes,” 2019. |
[20] | S. M. Cox, M. L. Williams, K. J. Leveno, “"The natural history of preterm ruptured membranes: what to expect of expectant management", Obstetrics and Gynecology,” pp. 558-562, 1988. |
[21] | J. C. Wilson, D. L. Levy, P. L. Wilds, “"Premature rupture of membranes prior to term: consequences of nonintervention", Obstetrics and Gynecology,” pp. 601-606, 1982. |
[22] | Maria Goya, “Premature rupture of membranes before 34 weeks managed expectantly: maternal and perinatal outcomes in singletons,” 2012. |
[23] | Delorme P, Goffinet F, Ancel P-Y, Foix-L&He ́lias L, Langer B, Lebeaux C, et al., “Cause of preterm birth as a prognostic factor for mortality. Obstet Gynecol 2016;127:40–8.,” 2016. |
[24] | Linehan LA, Walsh J, Morris A, Kenny L, O’Donoghue K, Dempsey E, et al., “Neonatal and maternal outcomes following midtrimes- ter preterm premature rupture of the membranes: a retrospec- tive cohort study. BMC Pregnancy Childbirth 2016;16:25.,” 2016. |
[25] | Yu H, Wang X, Gao H, You Y, Xing A., “Perinatal outcomes of pregnancies complicated by preterm premature rupture of the membranes before 34 weeks of gestation in a tertiary center in China: a retrospective review. Biosci Trends. 2015;9:35–41.,” 2015. |
[26] | Bendix JM, Hegaard HK, Bergholt T, Langhoff-Roos J., “Expectant management of PPROM and major complications before planned delivery: a retrospective cohort study. J Obstet Gynaecol 2015;35:570–7,” 2015. |
[27] | B.M Mercer, “"Premature Rupture of the Membranes", Obstetrics - Normal and problem pregnancies,” p. 713, 2007. |
[28] | Nguyễn Hữu Cốc., Ối vỡ non - ối vỡ sớm. Bài giảng Sản Phụ Khoa, Nhà Xuất Bản Y Học, 2006, pp. 129-132. |
N. S. D. D. M. e. a. Amuchou S. Soraisham, “"A multicenter study on the clinical outcome of chorioamnionitis in preterm infants",” American Journal of Obstetrics and Gynecology, pp. 372.e1-6, 2009. | |
[30] | Bukowski R, Hansen NI, Pinar H, Willinger M, Reddy UM, Parker CB, et al., “Altered fetal growth, placental abnormalities, and stillbirth. PLoS ONE 2017;12(8):e0182874.,” 2017. |
[31] | C. Nicaise, C. Gire, P. Fagianelli et al, “"Conséquences néonatales de la rupture prématurée des membranes entre 24 et 34 semaines d'aménorrhée : à propos de 118 grossesses uniques",” Journal De Gynécologie, Obstétrique Et Biologie De La Reproduction, pp. 747-754, 2002. |
[32] | the American College of Obstetricians and Gynecologists’ Committee on Practice Bulletins—Obstetrics, “ACOG PRACTICE BULLETIN No.80,” 2007. |
[33] | American College of Obstetricians and Gynecologists Committee on Obstetric Practice, “ACOG Committee Opinion No. 402: Antenatal corticosteroid therapy for fetal maturation,” 2008. |
[34] | B. M. Mercer, L. G. Crocker, N. M. Boe et al, “Induction versus expectant management in premature rupture of the membranes with mature amniotic fluid at 32 to 36 weeks: a randomized trial,” American Journal of Obstetrics and Gynecology, pp. 775-782, 1993. |
[35] | Joelle M. Lieman, Cynthia G. Brumfield, Waldemar Carlo et al, “Preterm premature rupture of membranes: is there an optimal gestational age for delivery?,” Obstetrics and Gynecology, pp. 12-17, 2005. |
[36] | R. Romero, S. Hanaoka, M. Mazor et al, “Meconium-stained amniotic fluid: a risk factor for microbial invasion of the amniotic cavity,” American Journal of Obstetrics and Gynecology, pp. 859-862, 1991. |
[37] | D. F. Lewis, C. D. Adair, J. W. Weeks et al, “A randomized clinical trial of daily nonstress testing versus biophysical profile in the management of preterm premature rupture of membranes,” American Journal of Obstetrics and Gynecology, pp. 1495- 1499, 1999. |
[38] | Brian M. Mercer, Yolanda A. Rabello, Gary R. Thurnau et al, “The NICHD-MFMU antibiotic treatment of preterm PROM study: impact of initial amniotic fluid volume on pregnancy outcome,” pp. 438-445, 2006. |
[39] | the American College of Obstetricians and Gynecologists’ Committee, “ACOG PRACTICE BULLETIN Clinical Management Guidelines for Obstetrician– Gynecologists No.217,” 2020. |
[40] | J. S.-S. J. M. e. a. A. Dhanya Mackeen, “Tocolytics for preterm premature rupture of membranes,” The Cochrane Database of Systematic Reviews, 2014. |
[41] | D. Roberts, S. Dalziel, “Antenatal corticosteroids for accelerating fetal lung maturation for women at risk of preterm birth,” The Cochrane Database of Systematic Reviews, 2006. |
[42] | J. E. Harding, J. Pang, D. B. Knight et al, “Do antenatal corticosteroids help in the setting of preterm rupture of membranes?,” American Journal of Obstetrics and Gynecology, pp. 131-139, 2001. |
Daniel Surbek, Gero Drack, Olivier Irion et al, “Antenatal corticosteroids for fetal lung maturation in threatened preterm delivery: indications and administration,” Archives of Gynecology and Obstetrics, pp. 277-281, 2012. | |
[44] | Sara Kenyon, Michel Boulvain, James P. Neilson, “Antibiotics for preterm rupture of membranes,” 2013. |
[45] | Từ Dũ, “Phác đồ chẩn đoán và điều trị Sản phụ khoa Bệnh viện Từ Dũ”. |
[46] | B. M. Mercer, M. Miodovnik, G. R. Thurnau et al, “Antibiotic therapy for reduction of infant morbidity after preterm premature rupture of the membranes. A randomized controlled trial. National Institute of Child Health and Human Development Maternal-Fetal Medicine Units Network,” pp. 989-995, 1997. |
[47] | Christian M. Briery, Edward W. Veillon, Chad K. Klauser et al, “Women with preterm premature rupture of the membranes do not benefit from weekly progesterone,” 2011. |
[48] | Saira Dars, Safia Malik, Irum Samreen et al, “Maternal morbidity and perinatal outcome in preterm premature rupture of membranes before 37 weeks gestation,” Pakistan Journal of Medical Sciences, pp. 626-629, 2014. |
[49] | Phạm Văn Khương., “Nghiên cứu cách xử trí ối vỡ non tại bệnh viện phụ sản trung ương năm 2008, trường Đại học Y Hà Nội, Hà Nội,” 2008. |
[50] | Lê Thu , “Nhận xét về xử trí và kết quả điều trị ra nước ối ở thai non tháng tại Bệnh viện Phụ sản Trung ương,” 2015. |
[51] | Vũ Thị Phương., “Thái độ xử trí ối vỡ non, ối vỡ sớm trên thai phụ con so đủ tháng năm 2009 và 2021, tại bệnh viện Phụ sản trung ương,” 2013. |
[52] | Nguyễn Quốc Hùng, “Tỷ lệ vô sinh và một số yếu tố liên quan đến vô sinh nam của các cặp vợ chồng được điều tra năm 2010 ở huyện Ba Vì,” Tạp chí Nghiên Cứu Học, 2012. |
[53] | Trần Đức Phấn, “Tình hình vô sinh ở Thanh Khê - Đà Nẵng,” Tạp chí y học thực hành, 2013. |
[54] | Vũ Thúy Hằng, “Nghiên cứu tỷ lệ vô sinh và một số yếu tố ảnh hưởng vô sinh tại tỉnh Cần Thơ năm 2009,” 2010. |
[55] | Nguyễn Đình Đông., “Nghiên cứu kết quả xử trí ối vỡ non, ối vỡ sớm giai đoạn IA ở tuổi thai từ 28 tuần tại bệnh viện phụ sản Trung Ương,” 2018. |
[56] | Oludag T, Gode F, Caglayan E, Saatli B, Okyay RE, Al- tunyurt S., “Value of maternal procalcitonin levels for pre- dicting subclinical intra-amniotic infection in preterm premature rupture of membranes. J Obstet Gynaecol Res 2014; 40: 954-60.,” 2014. |
[57] | Nasrin Asadi, Azam Faraji , Ameneh Keshavarzi , Mojgan Akbarzadeh-Jahromi, “Predictive value of procalcitonin, C-reactive protein, and white blood cells for chorioamnionitis among women with preterm premature rupture of membranes,” 2019. |
[58] | Ivana Musilova, Marian Kacerovsky , Martin Stepan, Tomas Bestvina, Lenka Pliskova, Barbora Zednikova, Bo Jacobsson, “Maternal serum C-reactive protein concentration and intra-amniotic inflammation in women with preterm prelabor rupture of membranes,” 2017. |
Samsudin I, Vasikaran SD., “Clinical utility and measure- ment of procalcitonin. Clin Biochem Rev 2017; 38: 59-68.,” 2017. | |
[60] | Cousens S, Blencowe H, Gravett M, Lawn JE. , “Cousens S, Blencowe H, Gravett M, Lawn JE. Antibiotics for pre-term pre-labour rupture of membranes: prevention of neonatal deaths due to complications of pre-term birth and infection. Int J Epidemiol. 2010;39(Suppl 1):i134–43.,” 2010. |
[61] | P. S. Ramsey, F. S. Nuthalapaty, G. Lu et al, “Contemporary management of preterm premature rupture of membranes (PPROM): a survey of maternal-fetal medicine providers,” American Journal of Obstetrics and Gynecology, pp. 1497-502, 2004. |
[62] | Joelle M. Lieman, Cynthia G. Brumfield, Waldemar Carlo et al, “Preterm premature rupture of membranes: is there an optimal gestational age for delivery?,” Obstetrics and Gynecology, pp. 12-17, 2005. |
[63] | Emre Baser, Demet Aydogan Kirmizi, Dilek Ulubas Isik, Safak Ozdemirci, Taylan Onat, Ethem Serdar Yalvac, Nihal Demirel & Ozlem Moraloglu Tekin, “The effects of latency period in PPROM cases managed expectantly,” 2020. |
[64] | Atalay Ekin; Cenk Gezer; Cuneyt Eftal Taner; Mehmet Ozeren; Ibrahim Uyar; Ibrahim Gulhan., “Risk factors and perinatal outcomes associated with latency in preterm premature rupture of membranes between 24 and 34 weeks of gestation,” 2014. |
[65] | Haiyan Yu, Xiaodong Wang, Haocheng Gao, Yong You, Aiyun Xing, “Perinatal outcomes of pregnancies complicated by preterm premature rupture of the membranes before 34 weeks of gestation in a tertiary center in China: A retrospective review,” 2015. |
[66] | N. Ilhan et al., “The relationship between the latency period, infection markers, and oxidant and antioxidant states in women with preterm premature rupture of membranes,” 2017. |
[67] | Mehmet Serdar Kutuk et al., “Relationship between maternal c-reactive protein level and neonatal outcome in patients with preterm premature rupture of membranes treated with Ampicillin and Azithromycin,” 2016. |
[68] | C. Nicaise, C. Gire, P. Fagianelli et al, “Conséquences néonatales de la rupture prématurée des membranes entre 24 et 34 semaines d'aménorrhée : à propos de 118 grossesses uniques,” Journal De Gynécologie, Obstétrique Et Biologie De La Reproduction, pp. 747-754, 2002. |
[69] | Cuu Nguyen Thien Thanh, Vo Minh Tuan, “ OUTCOMES OF PRETERM RUPTURE MEMBRANE AT THE GESTATIONAL AGE OF 28-34 WEEKS AND RISK FACTORS AT TUDU HOSPITAL (2007-2008),” 2009. |
[70] | Bộ Y Tế, Hướng dẫn chẩn đoán và điều trị Sản phụ khoa, 2015. |
[71] | The American College of Obstetricians and Gynecolgists, “Premature Rupture of Membranes,” Practice bulletin, 2016. |
[72] | Trần Quang Hiệp, “Nhận xét về tình hình đẻ non và một số yếu tố liên quan đến đẻ non tại Viện Bảo vệ bà mẹ và trẻ sơ sinh trong 3 năm 1998 – 2000, Luận văn Thạc sĩ y học, Trường Đại học Y Hà Nội, Hà Nội.,” 2001. |
[73] | Nguyễn Văn Phong., “Nghiên cứu tình hình đẻ non và một số yếu tố về phía mẹ và con liên quan đến đẻ non tại Bệnh viện Phụ Sản Trung Ương trong 2 năm 2001 – 2002, Luận văn Thạc sĩ y học, Trường Đại học Y Hà Nội, Hà Nội.,” 2003. |