123. Stevens T (2011), “Update on the role of endoscopic ultrasound in chronic pancreatitis”, Current Gastroenterology Reports, 13(2), pp.117- 122.
124. Teshima CW, Sandha GS et al (2014), “Endoscopic ultrasound in the diagnosis and treatment of pancreatic disease”, World Journal of Gastroenterology, 20(29), pp.9976-9989.
125. Tinto AL, Kang JY, Majeed A, Ellis C Williamson RC et al (2002), “Acute and chronic pancreatitis - diseases on the rise: a study of hospital admissions in England 1989/90-1999/2000”, Aliment Pharmacol Ther, 16(2), pp.2097-2105.
126. Tirkes T, Shah Z.K, Takahashi N et al (2019), Reporting Standards for Chronic Pancreatitis by Using CT, MRI, and MR Cholangiopancreatography: The Consortium for the Study of Chronic Pancreatitis, Diabetes, and Pancreatic Cancer, Radiology, 290(1), pp.207-215.
127. Tolstrup JS, Kristiansen L, Becker U, et al (2009), “Smoking and risk of acute and chronic pancreatitis among women and men: a population- based cohort study”, Archives of Internal Medicine, 169(6), pp.603-660.
128. Varadarajulu S, Eltoum I, Tamhane A, Eloubeidi MA (2007) “Histopathologic correlates of noncalcific chronic pancreatitis by EUS: a prospective tissue characterization study”, Gastrointestinal Endoscopy, 66(3), pp.501-509.
129. Vonlaufen A et al (2007), "Role of alcohol metabolism in chronic pancreatitis", Alcohol Research and Health, 30(1), pp.48-54.
130. Wallace MB, Hawes RH, Durkalski V, Chak A, Mallery S (2001), ”The reliability of EUS for the diagnosis of chronic pancreatitis: interobserver agreement among experienced endosonographers”, Gastrointestinal Endoscopy, 53(3), pp.294-299.
131. Wang LW, Li ZS, Li SD, Jin ZD, Zou DW, Chen F (2009), “Prevalence and clinical features of chronic pancreatitis in China: a retrospective multicenter analysis over 10 years”, Pancreas, 38(3), pp.248-254.
132. Weiss FU, Laemmerhirt F, Lerch MM (2019), “Etiology and Risk Factors of Acute and Chronic Pancreatitis”, Visc Med, 35(2), pp.73-81.
133. Whitcomb DC , Yadav D , Adam S et al (2008), “Multicenter approach to recurrent acute and chronic pancreatitis in the United States: the North American Pancreatitis Study 2 (NAPS2)”, Pancreatology, 8(4), pp.520-531.
134. Whitcomb D.C, Frulloni L, Garg P, Greer J.B, Schneider A, Yadav D, Shimosegawa T (2016), “Chronic pancreatitis: an international draft consensus proposal for a new mechanistic definition”, Pancreatology, 16(2), pp.218-224.
135. Whitcomb DC et al (2019), “Pancreatitis: TIGAR-O Version 2 Risk/Etiology Checklist With Topic Reviews, Updates, and Use Primers”, Clinical and Translational Gastroenterology, 10(6), pp. 10-27.
136. Whitcomb DC, Shimosegawa T, Chari ST, Forsmark CE et al (2019), “International consensus statements on early chronic Pancreatitis. Recommendations from the working group for the international consensus guidelines for chronic pancreatitis in collaboration with The International Association of Pancreatology, American Pancreatic Association, Japan Pancreas Society, PancreasFest Working Group and European Pancreatic Club”, Pancreatology, 18(5), pp.516-527.
137. Wiersema MJ, Hawes RH, Lehman GA, Kochman ML, Sherman S, Kopecky KK (1993), “Prospective evaluation of endoscopic ultrasonography and endoscopic retrograde cholangiopancreatography in patients with chronic abdominal pain of suspected pancreatic origin”, Endoscopy, 25(9), pp.555-564.
138. Wilcox CM, Yadav D, Ye T, Gardner TB, Gelrud A et al (2015), “Chronic pancreatitis pain pattern and severity are independent of abdominal imaging findings”, Clinical Gastroenterol Hepatol, 13(3), pp.552-560.
139. Wong T.S, Liao K.F, Lin C.M et al (2016), “Chronic Pancreatitis Correlates With Increased Risk of Cerebrovascular Disease A Retrospective Population-Based Cohort Study in Taiwan”, Medicine journal, 95(15), e3266
140. Yadav D, Timmons L, Benson JT, Dierkhising RA, Chari ST (2011), “Incidence, prevalence, and survival of chronic pancreatitis: a population-based study”, American Journal of Gastroenterology, 106(12), pp.2192-2199.
141. Yamabe A, Irisawa A, Shibukawa G, Abe Y et al. (2013) “Endosonographic Diagnosis of Chronic Pancreatitis”, Journal of Gastrointestinal and Digestive System, 2(5), pp.1-5.
142. Yamabe A, Irisawa A, Shibukawa G, Sato A, Fujisawa M (2017),”Early diagnosis of chronic pancreatitis: understanding the factors associated with the development of chronic pancreatitis”, Fukushima Journal of Medical Science, 63(1), pp.1-7.
PHỤ LỤC


Tổn thương ống tụy: sỏi ống tụy chính, giãn ống tụy, thành của ống tụy chính không đều, tăng âm thành ống tụy chính. Nhu mô tụy thấy các nốt và dải tăng âm. Chẩn đoán chắc chắn viêm tụy mạn với tiêu chí chính A và bốn tiêu chí phụ.
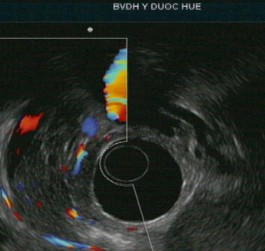
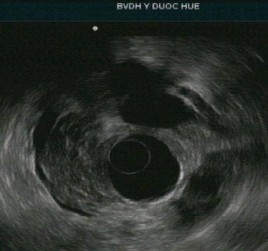
Tổn thương ống tụy: ống tụy chính không giãn nhưng có tăng âm thành ống tụy. Nhu mô tụy: tổn thương dạng tổ ong, các nốt tăng âm không có bóng lưng kèm các tổn thương trống âm. Chẩn đoán nghi ngờ viêm tụy mạn với 1 tiêu chí chính B kèm 3 tiêu chí phụ.
Số phiếu…………..
I. Hành chính
PHIẾU THU THẬP
Họ và tên: ..................................................Tuổi:.........................Giới: Nam/Nữ Địa chỉ: ......................................................................................................................
Nghề nghiệp: ................................................Dân tộc: ..............................................
Mã số bệnh nhân: ......................................................................................................
II. Phần nghiên cứu 1.Lý do vào viện
Đau bụng ![]() Sụt cân
Sụt cân ![]()
Rối loạn tiêu hóa ![]() Mệt mỏi, chán ăn
Mệt mỏi, chán ăn ![]() Nôn, buồn nôn
Nôn, buồn nôn ![]()
Khác: (Ghi rõ):................................................................................................
...................................................................................................................................
2.Tiền sử, bệnh sử 2.1.Bản thân
- Tiền sử uống rượu: Có ![]() Không
Không ![]()
Thời gian uống rượu: .....................................................................................
Số lượng rượu uống trung bình:.................................................... (đơn vị/tuần)
- Tiền sử nghiện thuốc lá:.................................................................... (gói.năm)
- Tiền sử mắc các bệnh lý liên quan:
...................................................................................................................................
...................................................................................................................................
...................................................................................................................................
...................................................................................................................................
2.2. Gia đình
...................................................................................................................................
...................................................................................................................................
...................................................................................................................................
3. Bệnh sử về triệu chứng đau bụng
Đau bụng: Có ![]() Không
Không ![]()
- Vị trí đau: Thượng vị ![]() Hạ sườn
Hạ sườn ![]() Quanh rốn
Quanh rốn ![]()
- Hướng lan: Không lan ![]() Lan ra sau lưng
Lan ra sau lưng ![]()
- Tính chất đau: Đau âm ỉ, liên tục ![]() Có cơn trội
Có cơn trội ![]()
- Yếu tố tăng đau: Sau ăn dầu mỡ ![]() Sau uống bia,
Sau uống bia, ![]()
- Tư thế giảm đau: Không ![]() Cò súng
Cò súng ![]()
- Mức độ đau: Chịu đựng được ![]() Thuốc uống
Thuốc uống ![]() Thuốc tiêm
Thuốc tiêm ![]()
4. Triệu chứng lâm sàng
- Buồn nôn: Có ![]() Không
Không ![]()
- Nôn: Có ![]() Không
Không ![]()
- Gầy sút, cân: Có ![]() Không
Không ![]()
- Ỉa lỏng: Có ![]() Không
Không ![]()
- Đi cầu phân mỡ: Có ![]() Không
Không ![]()
- Dấu hiệu vàng da: Có ![]() Không
Không ![]()
- Dấu hiệu thực thể khác: ................................................................................
...................................................................................................................................
...................................................................................................................................
...................................................................................................................................
5. Cận lâm sàng
Sinh hóa
Amylaze huyết thanh: .....................................................................................
Lipase huyết thanh: .........................................................................................
Glucose máu đói: ............................................................................................
Glucose bất kỳ.................................................................................................
HbA1c: ............................................................................................................
Chụp cắt lớp vi tính
Kích thước tụy: ...............................................................................................
Nhu mô tụy: Ngấm thuốc đồng nhất ![]() Không đồng nhất
Không đồng nhất ![]() Vôi hóa nhu mô: Có
Vôi hóa nhu mô: Có ![]() Không
Không ![]() Đầu tụy
Đầu tụy ![]() Thân tụy
Thân tụy ![]() Đuôi tụy
Đuôi tụy ![]()
Sỏi ống tụy chính: Có ![]() Không
Không ![]() Đầu tụy
Đầu tụy ![]() Thân tụy
Thân tụy ![]() Đuôi tụy
Đuôi tụy ![]()
Kích thước ống tụy chính: ..............................................................................
Số lượng sỏi ống tụy chính: ............................................................................
Tăng âm thành ống tụy: Có ![]() Không
Không ![]()
Các hình ảnh bất thường (nang tụy, u tụy, ống mật chủ bình thường hay giãn, túi mật to hay bình thường, bờ tụy đều hay không đều) ..................................
...................................................................................................................................
...................................................................................................................................
...................................................................................................................................
Phân loại Cambridge:
Cambridge 0: ![]() Cambridge 1:
Cambridge 1: ![]() Cambridge 2:
Cambridge 2: ![]()
Cambridge 3: ![]() Cambridge 4:
Cambridge 4: ![]()
6. Chẩn đoán viêm tụy mạn
![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
- Ống tụy
Có | Không | |
Giãn ống tụy chính | Có | Không |
Tổn thương không đều thành của ống tụy chính | Có | Không |
Giãn ống tụy nhánh | Có | Không |
Có thể bạn quan tâm!