The average age in my study is lower than foreign studies such as Jurkorvic's 35.5 years old [16]. This may be due to our country's habit of early marriage and early childbearing.
Research by Birge and colleagues showed that the older the age, the higher the rate of SMLT [46]. Recently, the rate of MLT has increased. According to research by Nguyen Huy Bao and colleagues, the rate of SMLT is common in women aged 20 - 34 [18]. Currently, many studies in the world are focusing on the age of the fetus, however, research on the age of the mother during pregnancy is also very meaningful in finding treatment directions, complications and accident rates during the implementation of the technique.
4.1.2. Obstetric history
In our study, we recorded that the number of subjects with 2 children accounted for the highest proportion at 65.1%. There were no cases with a history of premature birth. Regarding the number of previous miscarriages, there were 22 cases with no miscarriages, accounting for 25.6%, the rate of 1 miscarriage accounted for the majority at 30.2%. Among the 86 pregnant women studied, there was 1 case with 5 miscarriages. Some studies in the world also showed that many previous miscarriages are also one of the risk factors affecting unstable placenta. Among the children born to the study subjects, the number of children alive up to the present time accounted for a high proportion.
Number of miscarriages and abortions: 64/86 cases had miscarriages and abortions, accounting for 74.4%. Of these, 44.2% of patients had 2 or more miscarriages and abortions. A history of abortion and abortion can also be one of the risks leading to CSMLT in patients with previous MLT scars. Because when abortions are performed many times, the quality of the uterine muscle will be poor, the uterine cavity will be jagged, easily leading to pregnancy in a location other than the fallopian tube. When abortions can damage old surgical scars (especially in cases where the new scar is still loose, pregnancy in the old scar creates a large scar defect, making it easy for the fetus to nest).
Number of children: 56/86 patients (65.1%) had 2 children, the number of cases with 3 or more children was 17/86 (19.8%). There were no cases without children, the highest number of children was 4. The number of living children is one of the factors determining the treatment direction. For patients ≥ 30 years old, with enough children, previous surgery
After 2 or more times, the decision to perform open surgery to remove the pregnancy combined with sterilization or hysterectomy is easier. Because if the patient has had multiple MLTs and has enough children and is treated conservatively, the risk of pregnancy in SMLTs is higher in the following pregnancies or the risk of placenta accreta and uterine rupture in subsequent pregnancies. On the contrary, conservative treatment is always preferred in young cases and those who do not have enough children.
4.1.3. Number of cesarean sections
The study recorded the number of MLT at least 1 time, the most was 4 times. The group with the number of MLT at least ≥ 3 times, with 13 cases (15.1%) and the group with the most was 2 times, with 52 cases (60.5%). There were 3 cases ≤ 24 years old all had MLT 1 time. The study is similar to the results of some studies in the following table:
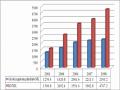
Table 4.2. Comparison of distribution by number of cesarean sections between studies
Number of cesarean sections
Author
1 time | 2 times | ≥ 3 times | ||
Jurkovic [16] | 2003 | 28% | 72% | |
Maymon [15] | 2004 | 37% | 63% | |
Dinh Quoc Hung [33] | 2011 | 51.6% | 45.6% | 2.8% |
Do Thi Ngoc Lan [47] | 2012 | 48.4% | 50% | 1.6% |
Ta Thi Thanh Thuy [34] | 2012 | 53% | 45% | 2% |
Diem Thi Thanh Thuy [32] | 2013 | 39.6% | 59.8% | 0.6% |
Nguyen Xuan Thuc [44] | 2017 | 30.6% | 58.1% | 11.3% |
Tran Thi Ngoc Ha [19] | 2021 | 37.5% | 51.1% | 11.4% |
Trieu Thi Phuong | 2022 | 34.4% | 50.5% | 15.1% |
Maybe you are interested!
-

 Internal control of revenue and expenditure activities at the National Children's Hospital - 2
Internal control of revenue and expenditure activities at the National Children's Hospital - 2 -
 Comparison of Imported Raw Materials Value and Export Turnover of Vietnam's Leather and Footwear
Comparison of Imported Raw Materials Value and Export Turnover of Vietnam's Leather and Footwear -
 Comparison of Number of Outpatients with More than 12 Times Medical Examination by Region
Comparison of Number of Outpatients with More than 12 Times Medical Examination by Region -
 Number of Credits: 3 (Theory: 2, Exercises: 1) – Time Distribution: 15 Weeks
Number of Credits: 3 (Theory: 2, Exercises: 1) – Time Distribution: 15 Weeks -
 Internal control of revenue and expenditure activities at the National Children's Hospital - 5
Internal control of revenue and expenditure activities at the National Children's Hospital - 5
The study recorded 13 cases (15.1%) of cesarean section 3 times or more, most of the pregnant women were between 30 - 39 years old, with 12/13 cases and this group had no cases ≤ 29 years old. This situation can be explained by the fact that this age group has not been pregnant many times and the normal birth rate of this group
quite high. Some of the reasons that have been investigated for the increase in the rate of CLT are social factors, CLT at the request of the mother and family. In 1991, 15.3% of newborns in Germany were CLT. By 2012, this figure was 31.7%. The increase in the rate of CLT is explained by the increasing tendency for pregnant women to not face the possible risks of vaginal delivery. Scientific advances in pregnancy diagnosis, socio-cultural changes also affect the rate of CLT. As CLT increases, the risks during and after CLT surgery must be considered, with complications affecting the next pregnancy, such as pregnancy in the old C-section scar. C-section is associated with risks for the mother and child, so C-section should only be performed when there are clear indications. Currently, there are not many studies investigating the relationship between MLT and the occurrence of pregnancy in SMLT in Vietnam as well as worldwide.
Many authors agree that the more times MLT is performed, the higher the pregnancy rate in old SMLT. This is explained by the fact that the more times the surgery is performed, the poorer the quality of the surgical scar, the more fibrous tissue there is, and the condition of creating a surgical wound defect creates an environment for the fetus to easily implant.
A study by the authors when analyzing the closure of the uterine muscle layers has an effect on limiting scar formation later. The time factor also contributes to the formation of gaps in the uterine muscle layer, affecting the attachment of the blastocyst and the SMLT defect is an easier place to nest. Another study noted that the more times MLT is performed, the higher the rate of pregnancy in SMLT. According to the study of Maymon et al., in 8 cases of pregnancy in SMLT, 63% of cases had a history of MLT more than twice [15]. According to Jurkovic et al., this rate is 72% of pregnancies in SMLT in cases of MLT more than twice [16]. Many evidences show a correlation between pregnancy in SMLT and the number of MLTs. Rotas 2006 study found that 52% of pregnancies on SMLT occurred in cases of MLT once, 36% in cases of MLT twice and 12% in cases of MLT more than 2 times [17].
However, it cannot be denied that some other studies have different results, even the opposite. That is, patients with pregnancy in old surgical scars are higher than those with a history of surgery once. This can also be explained.
that the current improved MLT method with the trend of single-layer uterine suturing can create a defect at the old MLT scar, making the quality of the uterine muscle at the incision thin, which is a favorable factor for CSMLT in the next pregnancy.
Through our research and the research referenced, it is found that there is still no consensus on the relationship between the number of MLT times and the rate of pregnancy after previous cesarean section. The reasons for this difference depend on the MLT rate, MLT method at each facility, postoperative care, nutritional quality, and genetic factors, so patients who have only MLT once have had a pregnancy after SMLT. Therefore, it is necessary to comply with the MLT technique, ensure hygiene in post-operative patient care, and improve the physical condition and nutrition of pregnant women after MLT. Women who have had MLT 2 or more times should be advised to have sterilization to reduce the risk of pregnancy after SMLT in subsequent pregnancies.
4.1.4. Distance from most recent cesarean section to present
The study noted that the group with a history of the most recent cesarean section over 24 months was the most common, accounting for 64 cases (74.3%). The least common group was the group under 6 months with 1 case accounting for 1.2%. The subject with the shortest recorded time was 5 months with the characteristic of being 37 years old and having a history of 2 cesarean sections. The subject with the longest time was 8 years with the characteristic of being 40 years old and having a history of 1 cesarean section.
Although the mechanism of SMLT is still unclear. According to a study, the most accepted pathogenesis is that the blastocyst attaches to the myometrium through a microscopic opening at SMLT or a surgical scar in the uterus. Currently, with the advancement of ultrasound, especially transvaginal ultrasound, hysterosalpingography, the integrity of the myometrium can be well determined in the absence of pregnancy.
A study by Smith A et al. in 2001 showed that if the interval from the most recent MLT to this SMLT pregnancy is < 18 months, the risk of uterine rupture during labor monitoring is 3 times higher than that of women with previous cesarean section > 18 months [48]. Therefore, hospitals from local to central levels often advise patients after MLT to avoid pregnancy for at least 1 year. In addition, due to psychological anxiety and poor economic conditions in rural areas, they are advised to avoid pregnancy.
pregnancy 2 years after CLT. Therefore, the study group had a high interval between 2 cesarean sections > 24 months.
4.2. Clinical and paraclinical characteristics of the study subjects
4.2.1. Clinical features
Delayed menstruation was the most common symptom, occurring in 53 cases, accounting for 61.6%. The patient with the longest amenorrhea symptom was 5 months. There were 48 patients with vaginal bleeding (accounting for 55.8%), 32 patients with abdominal pain (37.2%), 13 patients had no symptoms and the disease was only discovered by chance through ultrasound. Notably, there was 1 case admitted to the hospital with symptoms of hemorrhage, accounting for 1.2%.
Symptoms of lower abdominal pain were present in 32 cases, accounting for 37.2%. Symptoms of abdominal pain during pregnancy in SMLT were lower abdominal pain, dull pain and no different from abdominal pain symptoms in patients with threatened miscarriage or ectopic pregnancy.
Symptoms of abdominal pain may be accompanied by light vaginal bleeding or hemorrhage, this symptom occurred in 21 cases in our study. According to Nguyen Thi Kim Ngan's study, this rate is 13.6% [40], according to Tran Thi Thu Ha's study, the rate is 15.9% [19]. Symptoms of abdominal pain combined with vaginal bleeding are also common in CNTC and threatened miscarriage.
Our study recorded 1 case of hemorrhage (1.2%). When compared with some other domestic studies:
Table 4.3. Comparison of hemorrhage rates between studies
Author
Year | Rate (%) | |
Dinh Quoc Hung [33] | 2011 | 14.1% |
Ta Thi Thanh Thuy [34] | 2012 | 18% |
Diem Thi Thanh Thuy [32] | 2013 | 3.6% |
Nguyen Xuan Thuc [44] | 2018 | 4.8% |
Trieu Thi Phuong | 2022 | 1.2% |
The only case admitted to the hospital due to hemorrhage had the following characteristics: 7 weeks of pregnancy, during the abortion, bleeding was seen in the lower segment, a Foley catheter was inserted - 40ml of Betadin solution was injected into the catheter. After the procedure, the patient was stable and did not need to be transferred to surgery. The amount of blood lost during and after the procedure was about 400 ml.
According to Dinh Quoc Hung, the rate of hemorrhage is 14.1% [33], according to Ta Thi Thanh Thuy, it is up to 18% [34]. The rate of hemorrhage in the authors' study is much higher than our study because these two studies did not exclude cases of CSMLT that had been previously treated such as BTC curettage, medical abortion. This is the cause of hemorrhage. In our study, we only included cases of SMLT that had not been treated with any method before, so the rate of hemorrhage was lower.
Of the 48/86 patients with symptoms of vaginal bleeding, 4 were hospitalized due to prolonged bleeding. In these 4 cases, the shortest duration was 15 days, the longest was 2 months.
It can be seen that cesarean scar pregnancy has no specific symptoms. Therefore, it is difficult to diagnose cesarean scar pregnancy based solely on clinical symptoms. Pregnant women who have had cesarean scar surgery during pregnancy should be advised to have an early examination and ultrasound to detect cesarean scar pregnancy early if any.
4.2.2. Paraclinical characteristics
4.2.2.1. Pre-treatment β-hCG concentration
Before abortion, the rate of patients with the most common β-hCG concentration is
> 20000 mIU/ml accounted for 46/86 cases, equivalent to 53.5%. The least common β-hCG concentration was 10000 - 20000 mIU/mL, accounting for 20.9%. The highest pre-procedure β-hCG concentration was 398117 mIU/mL, the lowest was 74 mIU/mL. The average β-hCG concentration was 48287.9 mIU/mL.
In cases of pregnancy with β-hCG concentration > 300,000 mIU/mL, the physician must always consider the differential diagnosis of normal pregnancy or hydatidiform mole. In elderly women > 40 years old, the β-hCG concentration increases very high. If diagnosed with hydatidiform mole, special attention should be paid to placental cancer - primary cancer.
Choriocarcinoma or not. Chest X-ray to look for “balloon drop” image, regular β-hCG quantification during treatment.
β-hCG concentration > 20000 mIU/mL accounted for the majority with 53.5%. This result is equivalent to some studies:
According to Tran Thi Ngoc Ha: β-hCG concentration in the group of 10000 - 50000 mIU/mL has the highest rate of 55.7% [19]. According to Pham Thi Hai Yen, β-hCG concentration is most common in the range of 10000 - 50000 mIU/mL with 53.7% [49].
According to our study, the average pre-treatment β-hCG concentration was 48287.9 mIU/mL. This concentration according to Pham Thi Nhung's study was 56638.6 IU/L [50], according to Le Thi Anh Dao it was 2623.3 mIU/mL [9]. According to Wang
YL, this concentration is 24047 mIU/mL [29]. Thus, the pre-treatment β-hCG concentration has a fairly wide range of variation, which is closely related to the time of diagnosis of a pregnancy in the old SMLT.
According to Diem Thi Thanh Thuy, the concentration of β-hCG has little value in determining the treatment method, but only has value in monitoring and predicting during the treatment process. However, with small gestational ages, the lower the concentration of β-hCG, the higher the success rate of treatment.
4.2.2.2. Gestational age on ultrasound
According to the results of table 3.8, the group of gestational age < 6 weeks accounted for 19.8%; the group of gestational age from 6 weeks - < 9 weeks had 58 cases equivalent to 67.5% of which 32 cases had fetal heart activity. There were 11 patients with gestational age ≥ 9 weeks accounting for 12.8%. In this study, the youngest gestational age was 4 weeks, the oldest gestational age was 10 weeks and 6 days.
When comparing a number of studies:
According to Dinh Quoc Hung: gestational age < 6 weeks is 39%, gestational age 6 - 8 weeks 32%, gestational age > 8 weeks 14%, the youngest gestational age is 5 weeks and the oldest is 11 weeks [33]. According to Ta Thi Thanh Thuy: gestational age < 7 weeks: 69%, from 7 - 9 weeks 25%; over 9 weeks 5%, the youngest gestational age is 4.5 weeks, the oldest is 13 weeks, the average gestational age is 6.08 [34]. According to Nguyen Xuan Thuc: gestational age 8 - 10 weeks accounts for 43.5%
and the < 8 weeks group accounted for 41.9% [44].
According to foreign authors: the diagnosed gestational age is from 5 - 12 weeks, on average 7.5 ± 2.5 weeks. According to Jukovic, the diagnosed gestational age is from 4 - 23 weeks [16]. According to Timor - Tritsch, the diagnosed gestational age is from 6 - 14 weeks, of which the gestational age under 8 weeks accounts for 73% [35]. Thus, according to foreign authors, the gestational age is detected quite late due to the attempt to monitor the fetus until it is necessary to treat it, the gestational age is already large.
With the increasingly developed economic conditions and the increasingly improved educational level, women often go for early pregnancy check-ups. In addition, with the increasing development of diagnostic imaging equipment, fully trained medical staff help diagnose early pregnancy in the old SMLT.
However, some cases of gestational age are detected quite late because patients in remote areas do not go for early prenatal check-ups and there are a few cases of expecting children who try to monitor the pregnancy until they have to be treated, but the gestational age is already advanced. The earlier the gestational age is detected, the sooner the diagnosis and treatment can be easily done to avoid many complications.
Regarding the presence or absence of fetal cardiac activity on ultrasound. Our study recorded that the group with fetal cardiac activity and the group without fetal cardiac activity appeared at the same rate of 45 (52.3%) cases and 41 (47.7%) cases. This difference was not statistically significant, p > 0.05. The gestational age with fetal cardiac activity was recorded highest in the group ≥ 9 weeks and lowest in the group < 6 weeks. According to Nguyen Xuan, the gestational age with fetal cardiac activity was recorded at a high rate in the group from 6 weeks and above [44].
4.2.2.3. Location of the gestational sac:
Vial noted that pregnancy in SMLT progresses in two different directions [20]. The first type is the gestational sac attached to the surgical scar and develops toward the uterus. In this case, the gestational sac can progress until the fetus is full term but there is a risk of placenta accreta. The second type is the gestational sac deeply embedded in the surgical scar and progresses to cause uterine rupture in the first 3 months, causing massive bleeding that is life-threatening to the patient. Pathology shows that the placenta is attached to the lower segment without the uterine muscle layer and the decidua basalis, only a thin layer of connective tissue.