1.1.5. Normal liver density
The normal density of the liver without contrast injection ranges from 54-68UH, the blood vessels have a lower density, about 45UH.
1.2. Causes of CTG
There are many different causes of CTG such as: domestic accidents, work accidents, traffic accidents, etc. Of which, traffic accidents are the main cause of CTG, the rate in the study is from 59.8% - 71.6% [12].
Maybe you are interested!
-
 The Preposition “Auf” Viewed From a Cognitive Perspective Compared with Vietnamese
The Preposition “Auf” Viewed From a Cognitive Perspective Compared with Vietnamese -
 Example Illustrating a Summary of an English Text
Example Illustrating a Summary of an English Text -
 The relationship between travel motivation, destination image and destination choice - A case study of Binh Dinh province tourism destination - 1
The relationship between travel motivation, destination image and destination choice - A case study of Binh Dinh province tourism destination - 1 -
 Emotions of a first-time mother - 3
Emotions of a first-time mother - 3 -
 A Multifaceted View of Reality
A Multifaceted View of Reality
1.3. Clinical symptoms
Clinical diagnosis of CTG is often difficult due to nonspecific signs and easy to miss. In addition, CTG is often found in the context of multiple trauma with many combined injuries, especially traumatic brain injury and chest trauma, so clinical manifestations are often complex and atypical [9].
1.3.1. Systemic symptoms
Patients usually come to the hospital in a stable hemodynamic state, with normal pulse and blood pressure. In these cases, it is possible to continue monitoring and supplement diagnostic tests. On the other hand, when the patient comes to the hospital in a state of shock, hypotension, rapid pulse (small and difficult to detect), cold skin, sweating, even unconsciousness, with intra-abdominal bleeding syndrome, emergency surgery is needed to stop the bleeding [13].
1.3.2. Functional symptoms:
Most cases present with right upper quadrant abdominal pain that then spreads throughout the abdomen (due to parietal peritoneal irritation).
Vomiting or nausea and constipation may occur late after the accident.
1.3.3. Physical symptoms
- Bruises and abrasions on the right flank after impact.
- Abdominal bloating.
- Abdominal wall reaction, peritoneal sensation, abdominal wall stiffness.
In which, the rate of signs of skin abrasion in the liver area is from 43.97% - 46.1%, signs of abdominal distension with different levels appear at a rate of 61.8% - 67.7% [14].
Note examination to rule out associated injuries.
1.4. Paraclinical
1.4.1 Blood formula
Determining the patient's blood loss based on the results of red blood cell count, hemoglobin, and hematocrite is only partly valuable in assessing the amount of blood loss. Because after CTG, there is also a phenomenon of blood concentration and reduced circulating volume.
1.4.2. Blood biochemistry
Increased ALT, AST, Bilirubin is specific for liver cell damage.
1.4.3. Abdominal puncture
Several studies have found that paracentesis is no longer a good indicator for surgery and may lead to unnecessary surgery in 3–25% of cases [1,3].
1.5. Image exploration methods
1.5.1. Abdominal radiography without preparation
Unprepared abdominal radiography is almost no longer indicated in CTG.
- Direct signs: Enlarged liver shadow, uneven liver edges.
- Indirect signs: Fracture of the last right ribs. The diaphragm is pushed up, possibly collapsing the base of the right lung. The hepatic flexure of the colon is pushed. If there is intra-abdominal hematoma: a blurred image between the intestinal loops and the pelvic area [1].
1.5.2. Ultrasound.
Since the 1980s, ultrasound has been widely used in France, European countries and Japan to diagnose abdominal trauma [2]. In Vietnam and developed countries such as France and the US, the first examination that needs to be done for patients with blunt abdominal trauma is ultrasound [8]. On ultrasound, liver lesions can be seen: subcapsular hematoma, liver parenchyma contusion, liver rupture, free fluid in the abdominal cavity. In addition, ultrasound also helps assess the progression of contusion and hematoma in cases of conservative treatment [14]. The image of tissue contusion is shown by a heterogeneous hyperechoic area in the liver parenchyma, the image of hematoma in the parenchyma is shown by an anechoic area, or there may be a hematoma inside the contused liver parenchyma (shown by an hyperechoic image inside an anechoic image). The liver rupture is determined by an anechoic line in the tissue, however, the rupture is difficult to determine because it is obscured by blood clots.

Figure 1.6 : Hematoma in the parenchyma of the right liver lobe (arrow).
Source: Sato M., Yoshii H (2004) [15].
However, there are still some limitations in ultrasound: it depends a lot on the experience of the operator, has poor specificity in determining the source of bleeding, and is difficult in cases of thick abdominal wall, subcutaneous emphysema, abdominal distension, soft tissue crush injury or skin peeling [14].
1.5.3. Liver CT
Patients with stable hemodynamics and abdominal fluid on ultrasound should have a CT scan to assess the injuries. On the contrary, patients in shock who need emergency surgery and do not have time for a CT scan should have an ultrasound scan to find and orient the injured organ [17].
1.5.3.1. Shooting technique
Patient preparation
In case of emergency trauma, fasting is not required.
It is necessary to ask about the patient's history of allergy to drugs containing iodine and kidney failure, if any, to consider the benefits and risks of contrast injection.
Place the patient in a supine position with arms raised above the head to avoid image interference.
Instructions on how to hold your breath to avoid image interference due to movement while breathing. For multi-array detectors, the radiation time is very short, so patients may not need to hold their breath during the scan. This is very good in cases where it is impossible to hold your breath due to the following reasons: traumatic brain injury, coma, or combined chest trauma.
Shooting technique
Take pictures from the top of the diaphragm to the pubic symphysis.
Single-row scanners: Start scanning 45-60 seconds after contrast injection, slice thickness is 10mm, 8mm or 5mm consecutively and scans in a spiral pattern.
Multi-detector row scanners: Start scanning 70 seconds after contrast injection, slice configuration depends on the number of detectors 4x2.5 or 16x1.5, then slices can be reconstructed with arbitrary thickness and in different planes.
Examination process
Non-contrast CT scans are performed for the purpose of:
- Assess the density of liver parenchyma before injection
- Initially locate the lesion to perform the cutting layers after injection.
- Measure the density of the damaged area to assess blood perfusion after drug injection, detect blood clots with increased density naturally in the liver, around the liver and in the abdomen.
Post-contrast X-ray:
- The commonly used injection technique is rapid intravenous injection with a dose of 1-1.5ml/kg body weight.
- Fast intravenous injection speed 3ml-5ml/second with single-row receiver machine, 4-6ml/second with multi-row receiver machines.
Delayed post-injection imaging: at 120 seconds after injection in case of combined renal and excretory tract injury.
1.5.3.2. CTG images on CT scans
- Ascites: Free fluid in the abdomen is the most common image on CT of CTG patients [18]. A small amount of blood in the abdomen first appears in the space next to the bleeding site and when the amount of fluid increases, it will flow from Morison's space, along the colonic groove to the Douglas pouch [18].
- Subcapsular hematoma : On CT scan, subcapsular hematoma is a crescent-shaped or lens-shaped lesion, located between Glison's capsule and liver parenchyma, directly pressing on adjacent liver parenchyma. The density of the hematoma changes, initially increasing in natural density, from 60 - 80 UH, then gradually decreasing in density in the following days. After contrast injection, the hematoma does not increase in density [19].

Figure 1.7 : Subcapsular hematoma in the liver has a crescent shape (long arrow) or lens shape and hematomas in the liver parenchyma (short arrow).
Source: Shanmuganathan K, Mirvis SE [21].
- Parenchymal contusion : the contused liver parenchyma area often has uneven density reduction before contrast injection, and poor and uneven contrast uptake after injection. The size of the contusion area is very variable, it can be a limited area or widespread, occupying an area of the injured organ [21].

Figure 1.8 : Liver laceration and contusion – parenchymal hematoma (short arrow) in the area without peritoneal cover causing retroperitoneal hematoma (long arrow).
Source: Shanmuganathan K, Mirvis SE [21].
- Intraparenchymal hematoma: the lesion naturally increases in density from 60 - 80 UH, after contrast injection this area does not change in density. The center of the area
Contusions may contain hematomas that increase in density immediately after injury. Hematoma density also changes over time [21].
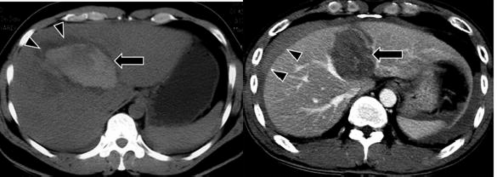
Figure 1.9 : Hematoma in the parenchyma before and after contrast injection (arrow).
Source: Shanmuganathan K, Mirvis SE [21].
- Liver parenchymal tear : also known as parenchymal rupture is a common type of liver parenchymal injury, which can be a simple tear or a complex tear of the parenchyma. The image on the CT scan is a continuous loss of parenchyma, a natural loss of density in the form of a straight line or tree branch before injection, after contrast injection the density does not change, the edges are irregular [21].
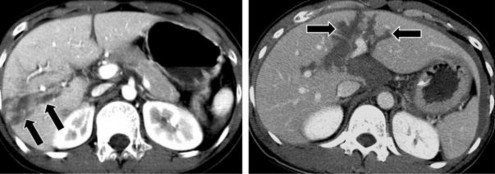
Figure 1.10 : Liver parenchymal laceration on CT scan (arrow).
Source: Shanmuganathan K, Mirvis SE [21].
- Infiltration around the portal vein : due to extravasation around the portal vein. On CT scan, this lesion is shown by the image of reduced density around the portal vein.
- Vascular damage: After injection, the contrast agent escapes from the blood vessels, forming a nodule or cluster located in the damaged liver parenchyma, increasing the density equivalent to the density of the vascular structure on the CT scan after arterial phase contrast agent injection [25].
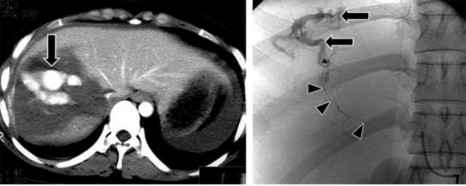
Figure 1.11 : Vascular damage (arrow).
Source: Shanmuganathan K, Mirvis SE [21].
- Hepatic vein injury: If the hepatic rupture passes through or approaches the hepatic veins, the veins are likely to be damaged [26].
- Portal vein damage: can be shown by the image of one or more lobes of the liver losing blood supply. Contrast-enhanced CT scan shows low-density liver areas around the portal vein and its branches.
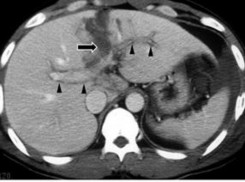
Figure 1.12 : Portal vein lesion on CT scan (arrow).
Source: Shanmuganathan K, Mirvis SE [21].