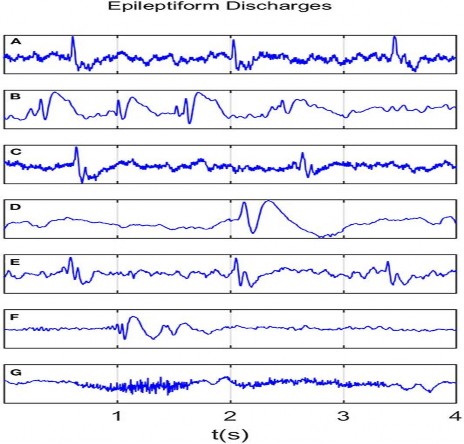
Figure 1.2 . Images of 7 types of epileptic seizures on EEG .
A: spike, B: spike and slow wave complex, C: spike, D: spike and slow wave complex, E: polyspike complex, F: polyspike and slow wave complex, G: polyspike rhythmic discharge. Source: Chong DJ, Hirsch LJ. J Clin Neurophysiol. 2005;22:79[24]
Figure 1.3. Generalized periodic attacks (GPDs)
Source: Chong DJ, Hirsch LJ. J Clin Neurophysiol. 2005;22:79[24]
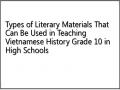
Figure 1.4. Right-sided periodic paroxysmal nodal attacks (LPDs)
Source: Chong DJ, Hirsch LJ. J Clin Neurophysiol. 2005;22:79[24]
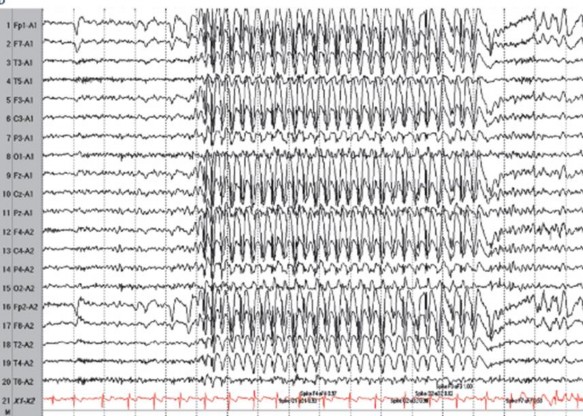
Figure 1.5. Electroencephalogram in generalized tonic-clonic seizures
Source: Chong DJ, Hirsch LJ. J Clin Neurophysiol. 2005;22:79[24]
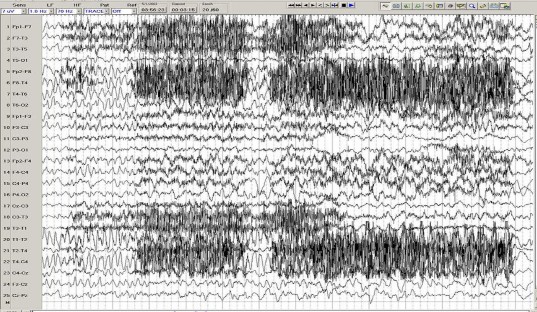
Figure 1.6. Electroencephalogram of partial seizure with right frontal temporal onset
Source: Chong DJ, Hirsch LJ. J Clin Neurophysiol. 2005;22:79[24]
1.1.4.2. Neuroimaging tests used in the diagnosis of epilepsy in pregnant women
Many countries and international organizations have their own guidelines for diagnostic imaging in pregnant patients. In 2017, the American College of Obstetricians and Gynecologists (ACOG) published "Guidelines for Diagnostic Imaging for Women During Pregnancy and Lactation" [25]. Although there are still some concerns about the unwanted effects of Magnetic Resonance Imaging (MRI) on pregnant women and fetuses (due to the induction of localized electric fields and electromagnetic currents in static or time-varying magnetic fields; due to the tissue heating effect of radiofrequency radiation), in fact, there have been no reports of serious effects due to MRI during pregnancy [25]. A study conducted on 1,737 pregnancies with MRI during pregnancy (compared with a control group of 1,418,451 births without MRI) showed that: MRI for pregnant women in the first trimester does not significantly increase the risk of stillbirth, neonatal death, congenital malformations, cancer, vision loss, or hearing loss in children (followed from birth to four years of age) [26]. On the other hand, studies on the safety of MRI for pregnant women and fetuses have mostly been performed at magnetic field strengths ≤ 1.5 Tesla. Animal studies
In pregnant women exposed to 3 Tesla magnetic fields, the heating effect was significantly increased in both amniotic fluid and fetal tissue [27]. However, a retrospective study of 81 newborns whose mothers had undergone MRI
3 Tesla during pregnancy showed no significant difference in mean birth weight or hearing loss at 12 months between the exposed and control groups [28]. In conclusion, magnetic head and neck MRI with a field of ≤ 3 Tesla is considered safe for both mother and fetus, providing many benefits in terms of diagnostic quality, but should only be performed when indicated by a neurologist [25].
Brain MRI is safer and more sensitive than brain CT for epilepsy. Brain MRI helps detect most of the lesions that cause epilepsy as well as provide images of normal brain structures , in addition to allowing multidimensional brain imaging and brain function assessment with many techniques.
different imaging. Therefore, brain magnetic resonance imaging is the neuroimaging study of choice for pregnant patients with epilepsy.
Causes of epilepsy related to brain structural abnormalities that can be detected on MRI include: hippocampal fibrosis, cortical developmental abnormalities, brain tumors, cerebral vascular malformations; cerebral infarction, cerebral hemorrhage; cerebral venous thrombosis; traumatic brain injury; central nervous system infections including: encephalitis, brain abscess, brain cysts [29],[30],[31].
Several abnormalities were detected on brain MRI.
|
Maybe you are interested!
-
 Types of lonely characters in contemporary Vietnamese prose through some typical works of Nguyen Huy Thiep, Ta Duy Anh, Chu Lai and Nguyen Danh Lam - 14
Types of lonely characters in contemporary Vietnamese prose through some typical works of Nguyen Huy Thiep, Ta Duy Anh, Chu Lai and Nguyen Danh Lam - 14 -
 For Exploiting Types of Tourism
For Exploiting Types of Tourism -
 Types of Literary Materials That Can Be Used in Teaching Vietnamese History Grade 10 in High Schools
Types of Literary Materials That Can Be Used in Teaching Vietnamese History Grade 10 in High Schools -
 Classification of the Convenience of 3 Types of Tourism
Classification of the Convenience of 3 Types of Tourism -
 Images of Artistic Space in Tay Poetry
Images of Artistic Space in Tay Poetry
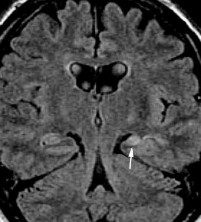
Figure 1.7. Left hippocampal fibrosis with left temporal lobe atrophy
Source: Hiba AH, Lawrence JH. Uptodate. 2018; Topic 14040 [29].
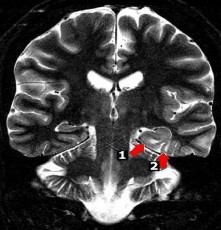
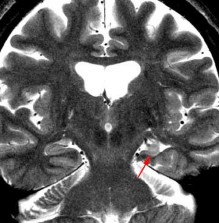
Figure 1.8. Focal cortical dysplasia in the left parahippocampal and occipitotemporal gyri
Source: Hiba AH, Lawrence JH. Uptodate. 2018; Topic 14040 [29].
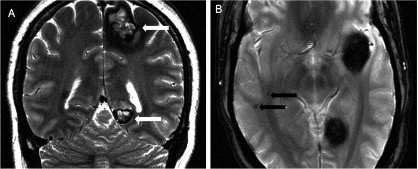
Figure 1.9. Familial cavernous malformation
Source: Hiba AH, Lawrence JH. Uptodate. 2018; Topic 14040 [29].
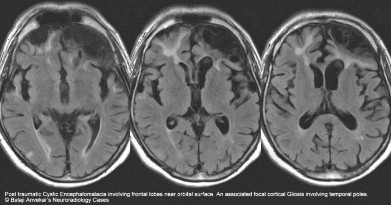
Figure 1.10. Brain injury after traumatic brain injury with cystic and focal gliosis
Source: Hiba AH, Lawrence JH. Uptodate. 2018; Topic 14040 [29].
Figure 1.11. Right frontal lobe lesion in Ramussen's encephalitis
Source: Hiba AH, Lawrence JH. Uptodate. 2018; Topic 14040[29].
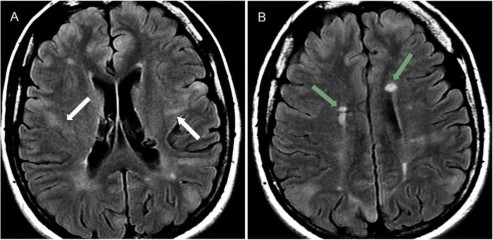
Figure 1.12. Brain lesions in tuberous sclerosis
Source: Hiba AH, Lawrence JH. Uptodate. 2018; Topic 14040 [29].
Figure 1.13. Brain damage in Sturge-Weber syndrome
Source: Hiba AH, Lawrence JH. Uptodate. 2018; Topic 14040[29].
Figure 1.14. Brain damage due to cerebral venous thrombosis
(Image provided by the author)
1.2. Studies on epilepsy in pregnant women
1.2.1. Research on maternal and child risk factors
1.2.1.1. Perinatal morbidity and mortality
Based on data collected in US hospitals (during the period from 2007-2011 with a group of 69,383 pregnant women with epilepsy and a control group of 20 million pregnant women without epilepsy) as well as the results of multiple analyses synthesized from many different studies, it shows that: Women with epilepsy have a higher rate of perinatal morbidity and mortality than the general population [32],[33],[34],[35]. Moderate to severe medical events occurring during this period include preeclampsia, premature birth, postpartum hemorrhage, stillbirth, fetal growth retardation and maternal death [32],[33],[34],[36]. Usually the frequency of each event is 1.1-1.5 times higher than the population, especially the mortality rate of pregnant women during labor is 10 times higher than the population [33],[34]. Clearly increased risk factors for women with epilepsy during the perinatal period include:
- Maternal mortality: there were 80 deaths per 100,000 women with epilepsy compared with 6 deaths per 100,000 women without epilepsy (adjusted OR 11.5; 95% CI: 8.6-15.1).
- The rate of cesarean section in the group of pregnant women with epilepsy was 41% compared with the population rate of 33% (OR 2.5).