- Rubber band ligation of hemorrhoids has been performed since the 19th century, but because the hemorrhoid is tied together with the skin around the anus, it is very painful after ligation, so it is not widely used. By 1958, Blaisdell had succeeded in tying only the hemorrhoid without the skin and surrounding tissues. Barron 1963 created a device to tie hemorrhoids with rubber bands and then with Mc Giveny's improved device, rubber band ligation of hemorrhoids became a successful treatment method for hemorrhoids and was the first choice among surgical treatments.
The main principle of rubber band ligation is to reduce blood flow to hemorrhoids, creating fibrous scar tissue that adheres to the muscle layer under the submucosa, thereby fixing the anal canal in accordance with the principle of preserving the anal cushion.
2.3.3. Infrared photocoagulation:
- The method of using heat to treat hemorrhoids has been practiced for hundreds of years. The goal of the coagulation method is to coagulate the tissue by the effect of heat, creating fibrous scars that reduce blood flow to the hemorrhoids and fix the hemorrhoids to the anal canal. With lasers, high-frequency electric currents also have a coagulating effect like infrared rays, but the accuracy of the penetration depth of the coagulation effect of these two methods is not as accurate as infrared rays with a coagulation machine. The tissue penetration of infrared rays is predetermined by adjusting the speed of the beam and the precise convergence on this tissue layer. The infrared coagulation machine has the advantage of not interfering with electronic devices attached to the patient such as pacemakers.
- Infrared photocoagulation is indicated for grade 1 and grade 2 internal hemorrhoids. This method has the advantage of being painless, safe, and very effective at stopping bleeding, but the disadvantage is that the machine is quite expensive and the procedure often requires multiple repetitions.
Maybe you are interested!
-

 Basic electronic engineering - City College of Construction. HCM Part 1 - 1
Basic electronic engineering - City College of Construction. HCM Part 1 - 1 -
 Basic Burn Rate Experimental Formulas
Basic Burn Rate Experimental Formulas -
 Basic Refrigeration Refrigeration and Air Conditioning Engineering - Intermediate - Ha Nam Vocational College 2020 - 1
Basic Refrigeration Refrigeration and Air Conditioning Engineering - Intermediate - Ha Nam Vocational College 2020 - 1 -
 Basic Conditions for Implementing Solutions
Basic Conditions for Implementing Solutions -
 Describe the causes of rickets.
Describe the causes of rickets.
2.3.4. Surgery:
- Surgical group 1: includes 2 surgical groups
+ Circular mucosal resection surgery:
Whitehead surgery: the principle is to cut the mucosa and submucosa with hemorrhoidal veins, then pull the mucosa from above down and suture it to the skin at the anus. This method is almost never used today because it leaves many serious complications such as anal stenosis, fecal incontinence and anal discharge. However, because of the radical nature of the surgery, many authors still use the principles of this surgery but modify it to reduce complications, for example, Toupet surgery.
+ Surgery to remove each hemorrhoid:
The principle of this surgery is to cut each hemorrhoidal mass separately, leaving skin-mucosal pieces (skin-mucosal bridges) between the hemorrhoids. This surgical group includes Milligan Morgan's surgery (1937), Ferguson's surgery (1959), Parks' surgery (1965), and Viet Duc Hospital's surgery (Nguyen Dinh Hoi, 1966).
This surgical group includes two main groups:
* Open hemorrhoidectomy: PT Milligan Morgan, PT Nguyen Dinh Hoi
* Closed hemorrhoidectomy: PT Ferguson.
This surgical group avoids the complications of the circular mucosal excision surgery group, but still has the disadvantages of postoperative pain, long hospital stay, late return to work time and is ineffective in cases of circular hemorrhoids.
- Surgical group 2:
Originating from the disadvantages of the Morgagni subcolumn surgery group and new discoveries in pathogenesis, since the 90s, based on the principle of preserving the anal cushion, reducing blood flow to the hemorrhoidal mass and reducing the volume of the hemorrhoidal mass, some new surgeries have been born with the principle of anal suspension such as Longo's PT, manual hemorrhoidal suture.
and the principle of reducing the volume of hemorrhoids such as hemorrhoidal artery ligation surgery under Doppler ultrasound guidance.
+ PT Longo (1993): Is a surgery using a circular stapler to cut a ring of mucosa on the dentate line 2-3 cm and suture the ring with a stapler. The principle of this surgery is to cut and suture the ring of mucosa, aiming to reduce blood flow to the hemorrhoidal venous plexus to reduce the volume of hemorrhoids and suspend the anal cushion into the anal canal. This method is popular because it is painless, has a short hospital stay, and allows the patient to return to work early. The disadvantage is that the cost is high, and the effectiveness has not been fully evaluated due to the short follow-up period.
Figure 82.8. Longo operation
+ Manual hemorrhoid suturing:
This is a modified method of Longo surgery in developing countries due to the high cost of Longo surgery. This method has been reported by Ahmed M Hussein, Nguyen Manh Nham, Nguyen Trung Vinh, Nguyen Trung Tin at conferences. This method is also based on the principle of Longo surgery, which is to reduce blood flow to the hemorrhoid to reduce the volume of the hemorrhoid and suspend the hemorrhoid to the anal canal by hand-sewn sutures to fold the mucosa on the 2-3 cm dentate line. This method was only reported after 2001.
+ Suturing of hemorrhoidal artery under Doppler ultrasound guidance (Figure 2):
This method was first performed by Kazumasa Morinaga in 1995, with a device called Moricorn, which is a machine consisting of a Doppler ultrasound probe attached to an anoscope, through which the author searched for 6 arteries, which are terminal branches of the superior rectal artery, and these arterial branches were sutured and tied at a position 2cm above the dentate line.
The principle of this method is to reduce blood flow to hemorrhoids, only applicable to grade 2 and 3 internal hemorrhoids, the advantage of this method is that it is painless and preserves the anal cushion.
All three of these methods do not address thrombosed internal hemorrhoids and cases with large skin tags.
VALUATION
Please choose the best answer for the following questions: Question 1 : Complications of hemorrhoids:
A- Constipation; hemorrhoidal thrombosis; sphincter dysfunction; anal infection.
B- Prolonged bleeding leading to anemia; hemorrhoidal thrombosis; sphincter dysfunction; anal fissure; anorectal fistula...
C- Prolonged bleeding; constipation; hemorrhoidal thrombosis, sphincter dysfunction; anal infection...
D- Constipation; prolonged bleeding leading to anemia; venous thrombosis; anal infection; anorectal fistula...
Question 2: Functional symptoms of hemorrhoids:
A- Bloody stools. Anal pain. Hemorrhoid prolapse. Difficulty defecating. B- Bloody stools. Anal pain. Hemorrhoid prolapse. Painful defecation.
C- Bloody stools. Feeling of heaviness and pressure in the anus. Hemorrhoid prolapse. Painful defecation. D- Bloody stools. Feeling of heaviness and pressure in the anus. Hemorrhoid prolapse. Difficulty defecating.
Question 3 : Physical symptoms of internal hemorrhoids:
A - Hemorrhoids often protrude, soft, flat, painless when pressed.
B - Ask the patient to push and see the hemorrhoids fall out of the anus, dark purple in color, in clumps, when pressed, the hemorrhoids flatten, become soft, and painless.
C - The anal area looks swollen, red, and painful when pressed. There may be yellow fluid leaking out.
D- Rectal examination or endoscopy to see red hemorrhoids. May be accompanied by proctitis and hemorrhoidal ulcers.
Question 4 : Treatment of large hemorrhoids at primary health care facilities: A- Insert medicine into the anus.
B- Send the patient to a higher level for thorough treatment. C- Ligate the hemorrhoids and use appropriate antibiotics.
D- Use topical anti-inflammatory drugs combined with laxatives.
Lesson 83
PHYSIOLOGY OF FERTILIZATION, IMPLANTATION AND DEVELOPMENT OF THE EGG
TARGET
1. Describe the physiology of conception.
2. Describe the movement and nesting of eggs.
3. Describe the development of eggs and egg appendages through two periods .
CONTENT
1. Physiology of conception
1.1. Definition of conception
- Fertilization: Is the combination of a male cell, the sperm, with a female cell, the egg, to form a developing cell called an egg (or zygote).
- Conception: Is fertilization followed by implantation of the egg.
- After nesting, the egg develops into the fetus and its appendages.
1.2. Spermatogenesis
- Testicular germ cells produce spermatogonia.
- From spermatogonia develop into spermatogonia I with 46 chromosomes.
- Through the process of mitotic division, the number of spermatocytes II has 23 chromosomes.
body
- From spermatocytes II, mitosis is divided into spermatozoa, then they develop.
Sperm develop with 23 chromosomes, including: 22 normal chromosomes and 1 sex chromosome X or Y.
- Each mature sperm consists of 3 parts: Head, body, tail.
+ Head: Oval, the front part has cytoplasm, the back part is a large nucleus containing chromosomes.
+ Body: in the middle is the axial cord, at the head is the centrosome.
+ Tail: Long in the middle with an axial wire.
Figure 83.1: Sperm
Sperm:
- Each ejaculation: 3 - 5 ml
- Sperm count: 60 - 120 million in 1ml of semen.
- Normal activity rate 60 - 80% of sperm move.
- Sperm live in the vaginal and uterine environment for about 3 days.
- Movement speed per minute 1.5 - 3mm
- Sperm are always produced from spermatogonia from adulthood to old age.
1.3. Oocyte
- From germ cells in the ovary form oocytes.
- When a baby girl is born, her ovaries have from 200,000 to 500,000 oocytes.
water
- From puberty to menopause, only 400 - 450 follicles mature, the rest regress.
atrophy
- From the primary oocyte develops into oocyte I with 46 chromosomes.
- Oocyte I divides into meiosis to give oocyte II and polar body I
- Each oocyte II divides into mitosis to give a mature oocyte and a polar sphere II. The mature oocyte gives 23 chromosomes. Of which, there are 22 normal chromosomes and 1 X sex chromosome.
- Oocyte diameter: 100 - 150 micrometers.
- The egg is released from the De Graff follicle, carrying surrounding granulosa cells.
around
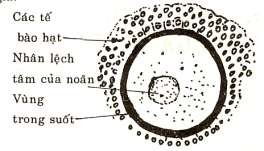
Figure 83.2: Structure of the oocyte
The structure of the oocyte has a shell called the zona pellucida. In the middle is the cytoplasm and nucleus.
When the egg is released, it is picked up by the fallopian tube and brought back to the fallopian tube.
The ovum survives in the fallopian tube for approximately one day.
1.4. Fertilization conditions include
- Sperm.
- Oocyte
- Vagina, cervix, uterus, fallopian tubes, ovaries are normal.
- Endometrial lining in pregnancy.
- Normal function of the gonads.
1.5. Fertilization mechanism
* Fertilization:
Occurs in the outer third of the fallopian tube. The sperm reaches the outer third of the fallopian tube, surrounds the oocyte, and then attaches to the zona pellucida of the oocyte. The sperm penetrates the zona pellucida to enter the cell. Usually only one sperm enters to fertilize, and only part of the head enters, the body and tail remain outside and atrophy.
* Changes in the nucleus:
The sperm head enters the oocyte, at first the male nucleus has chromosomes, then the oocyte releases polar sphere II to become a female pronucleus which also has chromosomes. If the fertilizing sperm carries the Y chromosome, the fetus will be a boy (XY fusion cell). If the fertilizing sperm carries the X chromosome, it will form an XX fusion cell, which will be a girl.
2. Egg movement and nesting
2.1. Movement of eggs
After fertilization, the egg moves through the fallopian tube into the uterine cavity. This movement is due to the effects of: The cilia of the fallopian tube lining, the peristalsis of the fallopian tube, and the fluid from the fallopian tube to the uterine cavity. The travel time is from 4 to 7 days.
During movement: The egg moves and grows. If for some reason the egg's movement is obstructed, the egg will stop and nest in the fallopian tube, causing an ectopic pregnancy.
2.2. Egg nesting
When the egg reaches the uterus, the uterine lining is prepared to receive the egg: The uterine lining has thickened due to the effects of Foliculin and Progesterone of the menstrual corpus luteum. This corpus luteum is maintained during the first months of pregnancy. The egg penetrates the outer layer of the uterine lining and burrows into the uterine lining to nest there and develop until full term.
3. Development of eggs and egg appendages
- After fertilization, the egg divides very quickly to form the fetus and its appendages.
pregnancy
- About time: Egg development is divided into 2 periods:
+ Organizational arrangement period: From fertilization to the end of the second month.
+ Complete organization period: From the 3rd month until full term.
3.1. Organizational arrangement period
3.1.1. Fetal formation
Immediately after fertilization, the egg divides very quickly. From one egg cell, it divides into 2 germ cells, then 4 germ cells, the cells divide equally. From 4 germ cells that divide unevenly into 4 large germ cells and 4 small germ cells, the large germ cells continue to divide and develop into a fetus with 2 layers of cells: the outer fetal layer and the inner fetal layer, between the 2 fetal layers, a middle fetal layer will later develop. These fetal layers form the embryo and then the fetus.
- External embryo: Forms nervous system, skin, bones, muscles
- Middle embryo: Forms circulatory system, urinary system, connective tissue
- Inner embryo: Forms respiratory and digestive systems
The fetus is shaped like a shrimp, and an umbilical sac develops on the abdomen of the fetus, which contains nutrients. Blood vessels are emitted into the umbilical sac to take nutrients to nourish the fetus. This is the first circulatory system, also known as the umbilical sac circulatory system.
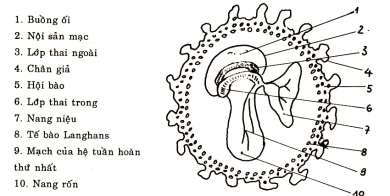
Figure 83.3: Comprehensive vegetable period
3.1.2. Development of appendages:
* Endometrial:
On the back of the fetus, some cells of the outer fetal layer dissolve to form a chamber called the amniotic cavity, which contains amniotic fluid. The wall of the amniotic cavity is a thin membrane called the endoplasmic reticulum.
* Mesentery:
- Small germ cells develop into mesoderm.
- The mesentery has two layers:
+ The outer layer is the endoplasmic reticulum.
+ The inner layer is Langhans cells.
- The mesoderm forms pseudopods that surround the egg.
* Peripartum:
When the egg nests, the uterine lining develops into the ectoderm, which is divided into three parts:
- Endometrial ectopy: Is the part related only to the uterus.
- Ovarian ectoderm: Is the part related only to the egg.
- Extrauterine-placental endometrial lining: Is the extramembranous part between the uterine muscle layer and the egg.
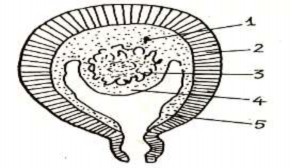
Figure 83.4: Endometrial ectopy
1. Endometrial-placental ectopic pregnancy.
2. Uterine muscles.
3. Eggs in the pre-placental period
4. Ovarian ectopy.
5. Endometrial ectopy.
3.2. Period of complete organization
3.2.1. Fetal development
- During this period, the fetus is called a fetus. The fetus has all the parts it needs to grow and complete its organization. During this period, the fetus lives by the urogenital circulatory system (called the second circulatory system).
- The blood vessels of the umbilical cyst develop towards the allantois to form a second circulatory system, while the allantois atrophies. Finally, the allantois circulatory system completely replaces the umbilical cyst. Gradually, the allantois also atrophies, leaving only the blood vessels, the umbilical artery and vein, to exchange nutrients from the mother's blood.
3.2.2. Development of appendages
* Endometrium: The endometrium grows to cover the amniotic fluid and fetus, and the amniotic sac expands.
* Mesentery:
The mesoderm becomes mostly smooth, developing only in the area attached to the uterus, here the mesoderm develops into chorionic villi with 2 cell layers: the synovial layer and Langhans. The small arteries entering each chorionic villi divide into capillaries with vascular walls close to the chorionic villi, blood returns to the umbilical vein to nourish the fetus.
* Peripartum:
The ectopic pregnancy gradually atrophies. The ectopic pregnancy also gradually atrophies. Near term, these two membranes fuse and become one, leaving only sparse patches. The ectopic pregnancy continues to develop and the blood vessels here dilate, forming a blood lake. In the blood lake, the mother's blood flows from the uterine artery branches. After exchanging nutrients, the blood follows the uterine veins back to the mother's circulation.
VALUATION
1: Describe the definition of conception? Explain the formation of the fetus in the period of organizational arrangement?
2: Describe the movement and nesting of eggs?
3: Describe the development of appendages during the organizational period?
4: Describe the development of the fetus and fetal appendages during the period of complete organization?
* Short answer questions from 5 to 10:
5: The structure of sperm consists of 3 parts: A:..........................................
B:............................................
C:...................................................
6: The fertilized egg moves to the uterus thanks to the following 3 factors: A:..........................................
B:............................................
C:...................................................
7: Fetal appendages include: A:..........................................
B:............................................
C:...................................................
8: There are 3 types of ectopic pregnancy: A: Ovarian ectopic pregnancy.
B:............................................
C:...................................................
9: After fertilization, eggs develop through 2 stages: A:..........................................
B:...................................................
10: The conditions for fertilization are: A:..........................................
B:............................................
C:...................................................
D: Endometrial lining in the gestational stage. E: Normal gonadal function.