Lesson 63
ACUTE APPENDICITIS
TARGET
1. Describe the clinical symptoms of acute appendicitis.
Maybe you are interested!
-
 Present the Causes, Epidemiology, Clinical Symptoms, Treatment and Prevention of Japanese Encephalitis.
Present the Causes, Epidemiology, Clinical Symptoms, Treatment and Prevention of Japanese Encephalitis. -
 Study on clinical features, pathology and treatment results of non-epithelial gastrointestinal cancer at Viet Duc Hospital - 17
Study on clinical features, pathology and treatment results of non-epithelial gastrointestinal cancer at Viet Duc Hospital - 17 -
 Clinical and paraclinical characteristics and treatment outcomes of patients with acute liver failure at the Poison Control Center of Bach Mai Hospital in 2020 - 2021 - 10
Clinical and paraclinical characteristics and treatment outcomes of patients with acute liver failure at the Poison Control Center of Bach Mai Hospital in 2020 - 2021 - 10 -
 Describe the Causes and Pathogenesis of Acute Pancreatitis.
Describe the Causes and Pathogenesis of Acute Pancreatitis. -
 Presenting Clinical Symptoms of Clavicle Fracture
Presenting Clinical Symptoms of Clavicle Fracture
2. Describe the dangerous complications of acute appendicitis.
3. Describe the treatment method for acute appendicitis at the primary health care level.
CONTENT
1. General
Appendicitis is a surgical emergency that occurs in all ages. It is the leading cause of abdominal emergencies. The disease requires early diagnosis and timely surgery. If diagnosed late and operated late, the disease will cause many dangerous complications and can be fatal. Therefore, when appendicitis is diagnosed or suspected, the patient must be transferred to a higher level facility early.

Figure 63.1. Location of the appendix:
a. Normal. b. Post-ileal
c. Post-cecum d. Small pelvis
2. Causes
Appendicitis can have the following causes:
2.1. Due to infection : Common bacteria are E. Coli, streptococcus, anaerobic bacteria.
2.2. Due to roundworms or fecal stones
2.3 . Due to constriction of blood vessels supplying the appendix, leading to malnutrition in the appendix, causing inflammation.
3. Symptoms
3.1. Systemic symptoms
Patients with infectious syndrome: Mild fever 38 o C to 38 o 5C, rapid pulse over 90 times per minute, dry lips, dirty tongue...
3.2. Functional symptoms
- Pain: Continuous dull pain localized in the right iliac fossa. Sometimes patients initially have pain in the epigastrium or around the navel and then localize in the right iliac fossa.
- Vomiting: Sometimes just nausea.
- Constipation, sometimes diarrhea.
3.3. Physical symptoms
Gently examine from the painless area to the painful area, and you can see:

Figure 63.2. Painful pressing on the right iliac fossa
- Pain in the right iliac fossa: pressing on the right iliac fossa, the most painful point is the appendix point (MacBurney point: The midpoint of the line connecting the navel to the right anterior superior iliac spine).
- Abdominal wall reaction in the right iliac fossa: This symptom is common and valuable.
treat
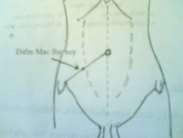

Figure 63.3. Mac-Burney point Figure 63.4. Rectal examination, right side pain
- Rectal and vaginal examination: press your finger into the right wall of the patient's rectum or vagina if it hurts.
3.4. Subclinical symptoms
- Blood test: High white blood cell count, in which the neutrophil ratio increased by over 70%.
- Ultrasound: Sees image of inflamed appendix (appendix increases in size, target shape, gloved finger shape)
4. Diagnosis
4.1. Definitive diagnosis
- Have infectious syndrome.
- Pain localized in the right iliac fossa.
- MacBurney point pain.
- There is abdominal wall reaction in the right iliac fossa.
4.2. Differential diagnosis
Examination to determine appendicitis is often difficult and easily confused with a number of diseases:
- Urinary tract diseases: Pain caused by right ureteral stones, urinary tract infections, right renal colic...
- Obstetric diseases: Ruptured ectopic pregnancy, ovarian cyst torsion, adnexitis...
- Digestive diseases: Peritonitis due to perforated gastric-duodenal ulcer, spastic colitis, intestinal perforation due to typhoid fever, Meckel's diverticulum.
- For other diseases: Right pelvic myositis, abdominal wall myositis ...
5. Complications

Figure 63.5. Appendicitis.
If not diagnosed and treated promptly, perforated appendix can cause dangerous complications.
Acute appendicitis that is not treated promptly can lead to complications.
after:
5.1. Peritonitis
This is a serious complication, usually after 24 to 48 hours the patient feels increased pain, pain spreading throughout the abdomen. Infection and poisoning increase markedly, constipation. There is peritoneal reaction.
5.2. Appendiceal abscess (Also known as localized peritonitis):
Due to untimely detection of appendicitis, the appendix ruptured, penetrating the greater omentum and surrounding organs to the surrounding abdominal cavity.
On examination, we found: There was a clearly defined tumor, adjacent to the right anterior superior iliac spine, the tumor surface was smooth, soft and painful to the touch. The patient's whole body still had a fever. Leukocytes increased.
5.3. Appendiceal mass
After a while the appendix becomes inflamed and is surrounded by the greater omentum and small intestine.
around
On examination, the infection syndrome will be reduced, and the pain will be less than before in the pelvic cavity.
There must be a hard plaque, unclear boundaries, little pain when pressed.
Figure 63.1. Progression of acute appendicitis.
Appendiceal mass
Acute appendicitis Peritonitis
appendiceal abscess
6. Treatment
Appendicitis requires early diagnosis and timely surgical treatment. When appendicitis is suspected or diagnosed, the following should be done:
* Principle of 3 no's:
- Do not inject painkillers.
- Do not inject into painful areas.
- No enema.
* Things to do:
- Explain to patient and family.
- Can be injected with booster (Vitamin B1 - Vitamin C).
- Patients should be transferred to higher level facilities as soon as possible.
VALUATION
Please choose the best answer for the following questions: Question 1 : General symptoms of acute appendicitis:
A- Patients with infection syndrome: Mild fever 38-38.5 0 C, rapid pulse > 90 times/minute, dry lips, dirty tongue...
B- Patients with toxic infection syndrome: High fever 39-40 0 C, rapid pulse > 90 times/minute, dry lips, dirty tongue, little urine or no urine...
C- Patients with toxic shock syndrome: Pale skin, pale mucous membranes, fatigue, rapid pulse, low blood pressure...
D- Patients with dehydration and electrolyte syndrome: Pale skin, pale mucous membranes, fatigue, rapid pulse, low blood pressure...
Question 2 : Pain symptoms in acute appendicitis:
A- Sudden, severe pain localized in the left iliac fossa. Sometimes patients initially have pain in the epigastrium or around the navel, then localized in the left iliac fossa.
B- Dull, intermittent pain localized in the left iliac fossa. Sometimes patients initially have pain in the epigastrium or around the navel, then localized in the left iliac fossa.
C- Continuous dull pain localized in the right iliac fossa. Sometimes patients initially have pain in the epigastrium or around the navel, then localized in the right iliac fossa.
D- Sudden, severe, intermittent pain localized in the right iliac fossa. Sometimes patients initially have pain in the epigastrium or around the navel, then localized in the right iliac fossa.
Question 3 : Diagnosis of acute appendicitis:
A- There is an infectious syndrome. Pain is localized in the left iliac fossa. Macbutney point is painful. There is abdominal wall reaction in the left iliac fossa.
B- There is an infectious syndrome. Pain is localized in the right iliac fossa. Macbutney point is painful. There is abdominal wall reaction in the right iliac fossa.
C- Dehydration and electrolyte syndrome. Pain localized in the left iliac fossa.
D- Dehydration and electrolyte syndrome. Pain localized in the right iliac fossa. Macbutney point is painful. There is abdominal wall reaction in the right iliac fossa.
Lesson 64
STOMACH PENETRATION
TARGET
1. Describe the clinical symptoms of gastric perforation.
2. Describe the dangerous complications of gastric perforation.
3. Describe the initial treatment of gastric perforation at primary health care facilities.
CONTENT
Perforation of the stomach and duodenum is often a complication of peptic ulcers. When perforated: fluid, food, and gas from the stomach flow into the abdominal cavity. If not operated on promptly, the patient will die after 3-5 days. Therefore, early detection of the disease and transfer of the patient to a higher level is important.


Figure 64.1. Lesser curvature perforation Figure 64.2. Duodenal perforation
1. Cause
1.1. Main cause : Chronic gastric and duodenal ulcers.
1.2. Rare causes
- Perforated ulcers (Curlinh ulcers) in the stomach, duodenum, in burn patients, after trauma.
- Or patients on long-term Corticoid treatment (such as Prednisolone ...... )
1.3. Favorable conditions
- Common disease in alcoholics.
- When the weather changes, it happens a lot in winter and spring.
- Due to injury.
- Common age: 30 - 50 years old.
- Gender: Men are more likely to have this condition than women.
2. Pathology
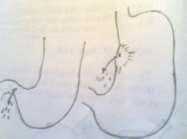
Figure 64.3. Pyloric perforation, lesser curvature
2.1. Common location : Duodenum or lesser curvature.
2.2. Hole
- Quantity: Mostly 1 hole. In some cases 2-3 holes may be encountered.
- Size: The hole is as small as a green bean, some are as big as a thumb. The edge of the perforated ulcer is calloused, hard but crumbly.
2.3. Abdominal condition
The degree of abdominal dirtiness depends on whether the perforation is near or far from the meal or whether the perforation is small or large, and whether the patient can be hospitalized sooner or later.
3. Clinical symptoms
3.1. Systemic symptoms
- Patients are susceptible to shock due to pain: rapid pulse, low blood pressure, cold limbs, sweating, difficulty breathing, shock usually lasts 30 minutes to 1 hour after which pulse and blood pressure improve.
- If you come early in the first hours, there will be no signs of infection. If you come late, there will be signs of infection or poisoning: rapid pulse, low blood pressure, gaunt face, little or no urine.

Figure 64.4. Stabbing pain and vomiting in late onset.
3.2. Functional symptoms
3.2.1. Pain : Sudden, severe, stabbing pain in the epigastric region then spreading throughout the abdomen. The pain makes the patient afraid to breathe heavily and move.
3.2.2. Vomiting : rare.
3.2.3. Constipation: Usually occurs 12 – 24 hours after perforation.
3.3. Physical symptoms


Figure 64.5. Abdominal X-ray KCB Figure 63.6. Abdominal wall examination
3.3.1. Look:
- The patient always bends over and holds his stomach with both hands.
- Abdomen is distended and does not move with breathing.
3.3.2. Palpation: Abdominal wall is hard as wood.
3.3.3. Percussion: The anterior hepatic dullness is gone and the 2 iliac fossae are dull.
3.3.4. Rectal and vaginal examination : When pressing a finger into the Douglas pouch, the patient feels pain.
3.4. X-ray
Abdominal X-ray without preparation in standing position: 75% show air crescent under the diaphragm.

Figure 64.7. Image of air crescent under the diaphragm
4. Diagnosis
4.1.Definitive diagnosis
- Patients with a history of gastric or duodenal ulcers.
- Sudden, severe abdominal pain in the epigastric region and pain spreading throughout the abdomen.
- Abdominal wall stiffness.
- X-ray shows a crescent shape below the right diaphragm.
4.2. Differential diagnosis:
- Peritonitis due to perforated appendix: The first pain point is in the right iliac fossa.
- Biliary peritonitis: Symptoms include pain, fever, and jaundice.
- Peritonitis due to typhoid intestinal perforation: Patients often have high fever lasting for many days followed by sudden, severe abdominal pain.
- Intestinal obstruction: The patient has intermittent abdominal pain, vomiting and constipation, with prominent intestinal loops.
- Ruptured ectopic pregnancy : History of amenorrhea, initial pain in the lower abdomen and anemia
5. Complications
5.1. Localized peritonitis ( subdiaphragmatic abscess).
5.2. Generalized peritonitis
5.3. Infection, poisoning due to late arrival
5.4. Renal failure
5.5. High mortality rate: If the patient presents late and is common in the elderly.
Figure 64.1. Progression of peritonitis
Poisoning
Localized peritonitis
(subdiaphragmatic abscess)
Generalized peritonitis
Kidney failure
Death
6. Treatment at primary health care facilities
Patients need to be quickly transferred to a higher level while still in good condition for emergency surgery.
6.1. Things to do
- Place a gastric tube.
- Infusion if available.
- Inject cardiac stimulant.
- Located in a cool place in summer and warm in winter.
- When the shock is over, transfer the patient to a higher level.
6.2. Things not to do
- No food or drink allowed.
- Do not inject painkillers.
- Do not inject into the abdominal wall.
- Do not douche .
VALUATION
Please choose the best answer for the following questions: Question 1 : The main cause of stomach perforation:
A- Due to acute perforation of gastric-duodenal ulcers, in burn patients, after trauma...
B- Due to perforation of chronic ulcers in the stomach or duodenum. C- Usually due to trauma to the stomach area.
D- Often seen in patients receiving long-term Cocticoid treatment.
Question 2: Physical symptoms of gastric-duodenal perforation:
A- Look: The patient is always bent over, holding his stomach with both hands. The stomach is soft and moves with breathing.
Palpation: Distended intestinal loops.
Percussion: The anterior hepatic dullness is gone, and the two iliac fossae are dull.
Rectal-vaginal examination: Duglas pouch is painful to press.
B- Look: The patient is always bent over, with both hands holding the abdomen. The abdomen is soft and moves with breathing.
Palpation: Abdominal wall is hard as wood.
Percussion: The anterior hepatic dullness is gone, and the two iliac fossae are dull.
Rectal-vaginal examination: Duglas pouch is painful to press.
C- Look: The patient is always hunched over, holding his stomach with both hands. The stomach is distended and does not move with breathing.
Palpation: Abdominal wall is hard as wood.
Percussion: The anterior hepatic dullness is gone, and the two iliac fossae are dull.
Rectal-vaginal examination: Duglas pouch is painful to press.
D- Look: The patient is always hunched over, holding his stomach with both hands. The stomach is distended and does not move with breathing.
Palpation: Abdominal distension, prominent intestinal loops.
Percussion: The anterior hepatic dullness is gone, and the two iliac fossae are dull.
Rectal-vaginal examination: Duglas pouch is painful to press.
Question 3: Paraclinical tests have diagnostic value for gastric-duodenal perforation:
A- Unprepared abdominal X-ray in standing position with 70% flexion shows a crescent of air under the diaphragm.