in the process of food digestion, blood filtration and anti-infection . HBV has 3 types of antigens HBsAg, HBeAg and HBcAg, corresponding to the 3 types of antigens above are 3 types of antibodies anti-HBs, anti-HBc and anti-HBe. The presence of these antigens and antibodies is important in determining the disease, disease type as well as disease progression.
The disease can be transmitted through blood, sexual contact, and from mother to child. If the mother is infected with HBV and has HBeAg (+), the possibility of transmission to the child is more than 80% and about 90% of children born will have chronic HBV. Hepatitis B virus can develop acutely, in which more than 90% of cases recover completely, nearly 10% progress to chronic hepatitis and the final consequence is cirrhosis or liver cancer [41], [59].
Diagnosis of HBV infection is mainly based on the detection of HBsAg surface antigen in serum. HBsAg can appear as early as day 6 after exposure, but is most clearly identified in weeks 4 to 8. HBsAg may be the only sign in acute HBV infection. HBsAg surface antigen can persist for several weeks, sometimes up to 3 months in patients who have recovered from acute HBV infection.
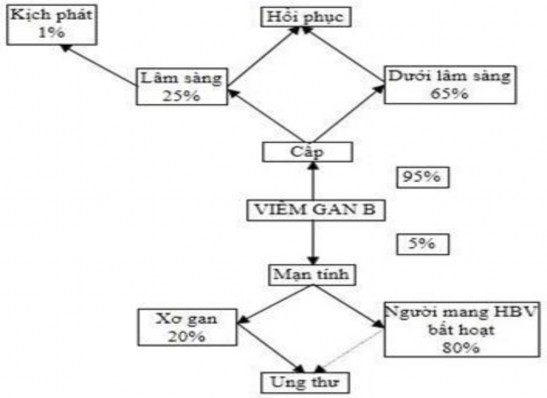
Figure 1.1. Diagram of the harmful effects of HBV infection and HBV disease [ 60]
1.3.1.2. Definition, diagnosis, and assessment of occupational hepatitis B virus
Occupational hepatitis B is a hepatitis caused by the hepatitis B virus during work. Common occupations and sources of exposure to HBV include health care workers; prison guards; police officers and other occupations and jobs exposed to the hepatitis B virus. Health care workers can be infected with HBV during the provision of health care services such as patient care, testing, and disease prevention.
According to Circular No. 15/2016/TT-BYT dated May 15, 2016 of the Minister of Health on Guidelines for diagnosis and assessment of reduced working capacity due to occupational hepatitis B virus, the minimum exposure limit for workers diagnosed and assessed with occupational hepatitis B is the causative factor recorded in the occupational exposure assessment section of the Work Environment Monitoring Results Report or the confirmation record.
exposure to harmful factors causing acute occupational diseases according to current regulations in case of occupational accidents. The minimum exposure time to a source of HBV infection is 1 time. The time to ensure that workers after exposure to a source of HBV infection are diagnosed with occupational hepatitis is prescribed for acute hepatitis: 6 months; chronic hepatitis: 2 years; cirrhosis: 20 years; and liver cancer: 30 years.
To diagnose occupational hepatitis B, it is necessary to base on occupational exposure factors, exposure time, guarantee time, clinical and paraclinical symptoms as prescribed in Appendix 30 of Circular 15. To assess the level of physical damage (%) of workers with occupational hepatitis B, it is necessary to base on the disease types and stages of progression when there is a history of hepatitis; chronic hepatitis; cirrhosis; liver cancer and impaired liver function. It is necessary to differentiate acute viral hepatitis B from other types of hepatitis such as: toxic hepatitis, hepatitis caused by other viruses (hepatitis A, hepatitis E, hepatitis C), autoimmune hepatitis, alcoholic hepatitis [61], [62].
1.3.2. Hepatitis C virus
1.3.2.1.Definition of disease, transmission route and diagnosis of hepatitis C
Hepatitis C is a liver infection caused by Hepatitis C Virus (HCV). The disease progresses silently, is long-term and causes serious consequences: cirrhosis occurs in 20-30% after 10-20 years, liver cancer occurs annually in 2-5% of chronically infected people. Any healthcare worker can be infected with HCV due to contact with HCV patients during work [41],[63].
HCV is a blood-borne pathogen with a worldwide prevalence of approximately 2.35% (estimated 160 million people). In developed countries, the most common route of HCV infection is intravenous drug use, in developing countries by invasive procedures, treatment by injection through infected skin. Without treatment, most
Acute infections all progress to chronic infections, cirrhosis, and liver cancer [64], [65].
HCV can cause acute and chronic hepatitis. Acute HCV infection is usually asymptomatic, accounting for about 50-90% of cases. HCV infection cannot be cured naturally in 50-90%, depending on the symptoms of the disease, age at infection and the route of transmission. HCV infection is a public health problem worldwide. HCV is a serious infectious disease and can lead to disability or death. Significant costs are incurred for prevention and treatment of HCV and the consequences of chronic progression of the disease, causing health problems, loss of work capacity and premature death. According to WHO, about 150 million people worldwide are chronically infected with HCV and hepatitis C is the cause of 350,000 deaths annually. HCV is mainly transmitted through contact with infected blood due to skin or mucosal injury. Acute HCV infection is often asymptomatic and therefore often overlooked. In 80% of patients, the clinical course is chronic, leading to an increased risk of developing cirrhosis or hepatocellular carcinoma. Risk factors for HCV infection include intravenous injection and blood transfusion or contact with an infected patient through an open wound. There is no vaccine or pre-exposure prophylaxis for HCV infection [66], [67], [68].
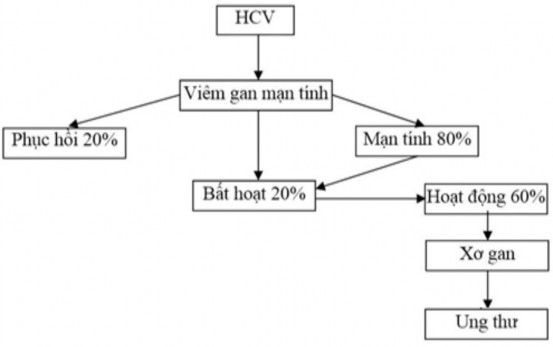
Figure 1.2. Diagram of the harmful effects of HCV infection and VGC disease [ 40]
1.3.2.2. Definition, diagnosis, and assessment of occupational hepatitis C virus
Occupational hepatitis C is hepatitis caused by the hepatitis C virus during work. The causative factor is exposure to the hepatitis C virus during work. Common occupations and sources of exposure to HCV include health care workers; prison guards, police officers, and other occupations and jobs that expose them to the hepatitis C virus.
The minimum exposure limit for workers diagnosed and assessed with occupational hepatitis B is the causative factor recorded in the occupational exposure factor assessment section of the Work Environment Monitoring Report or the record confirming exposure to harmful factors causing acute occupational diseases according to current regulations in case of occupational accidents. The minimum exposure time to a source of HCV infection is 1 time. The time to ensure that workers after exposure to a source of HCV infection are diagnosed with occupational hepatitis B is prescribed for acute hepatitis.
6 months; Chronic hepatitis is 2 years; Cirrhosis is 20 years; and Liver cancer is 30 years.
To diagnose occupational hepatitis C, it is necessary to base on occupational exposure factors, exposure time, guarantee time, clinical and paraclinical symptoms according to regulations in Appendix 33 of Circular 15 [61].
1.3.3. Current status of hepatitis B and C virus in medical staff
1.3.3.1. Research in the world
HBV infection occurs worldwide, most commonly in countries in Asia and Africa. HBV is closely associated with cirrhosis and primary hepatocellular carcinoma. Currently, there are approximately 300 - 400 million people carrying HBV worldwide. It is estimated that each year, approximately 1 to 2 million people die from the consequences of long-term HBV infection [69], [70], [71].
In Vietnam, according to a study in Ho Chi Minh City in 2005 on the rate of HBsAg carriers in 9078 people, the distribution was uneven by age. Children aged 1-3 had a positive rate of HBsAg of 7.8%; 4-6 years old: 10.3%. 7-10 years old: 12.2%; the groups aged 11-15 and 16-20 years old had an equal rate of 13.3%; The two groups aged 21-30 and 31-40 years old had a positive rate of HBsAg of 16.3%; the highest was the age group of 41-50 with 18.7% of people carrying HBsAg (+); in the age group over 60, this rate decreased to 13.4%. Thus, the rate of HBsAg carriers increases with age and this distribution result is similar to that in other localities in Vietnam.
Medical staff are in contact with patients in medical facilities during examination, treatment, and diagnostic testing, so they often face the risk of exposure to blood and secretions of patients carrying HBV and HCV. In reality, there are many risk factors that can cause skin damage in hospitals: subcutaneous injections, glass fragments, sutures, butterfly needles, drills, blood sampling, etc. According to WHO, in Europe, each year 304,000 medical staff are exposed to HBV, 149,000 medical staff are exposed to HCV, 22,000 medical staff are exposed to HIV and are at risk of
The risk of infection after occupational exposure is < 0.3-4.4% for HIV, 0.5-39% for HCV, and 18-37% for HBV [40], [72]. According to WHO estimates, nearly 40% of HBV infections in HCWs are due to occupational infection. It is estimated that every year, 30 out of 100 nurses have at least one needlestick injury, and each needlestick injury has the highest risk of HBV infection (up to 30%) compared to HCV and HIV [34].
According to a study by Olorunfemi Akinbode Ogundele et al. in 2017 on the status of infection and knowledge of hepatitis B and C among health workers at a specialist hospital in the Southwest, Nigeria. The study was conducted on 209 health workers, the results showed that the rate of HBsAg infection was 6.7%, the prevalence of HCV was 8.1%, and HBV and HCV co-infection was ± 0.1%, knowledge of hepatitis B in the study subjects was 80.0%, hepatitis C was 75.6%. Some factors related to HBV and HCV infection such as working time and knowledge [73].
Adriana Garozzo's research group (2017) conducted a 10-year study to determine the prevalence of HCV infection among HCWs from a health facility. A health surveillance program tailored to 3,138 HCWs working in four Italian health facilities was implemented. HCV infection was detected in 229 of 3,138 HCWs (7.3%). Among the HCWs infected with HCV, 43% were nurses, 34% were physicians and surgeons, and 23% were other staff. An important result of the study was that during the 10-year survey, there were no new cases of HCV infection among the HCWs monitored. These results emphasize the concept that correct handling procedures for hazardous specimens and the use of personal protective equipment, frequent hand washing, and care when handling biological materials, needles, or sharp objects lead to reduced or complete avoidance of the risk of infection from specimens containing infectious microorganisms [74].
1.3.3.2 Research in Vietnam
In Vietnam, according to the report on occupational health activities and occupational disease prevention of the Department of Health Environment Management, up to 2016, there were 34 types of occupational diseases insured, of which the group of occupational diseases caused by microorganisms had 5 diseases, including: Occupational tuberculosis; Occupational leptospirosis; Occupational hepatitis B; Occupational hepatitis C and HIV infection due to occupational accidents. Up to now, out of a total of more than 28,000 workers compensated for occupational diseases, there were 397 cases of occupational diseases caused by microorganisms, accounting for the lowest rate (1.43%) among the 5 groups of occupational diseases insured in Vietnam. Detailed statistics are presented in the following table [75]:
Table 1.1. Statistics of occupational diseases caused by microorganisms in Vietnam [75]
Occupational diseases caused by microorganisms
1991- 2000 | 2001- 2005 | 2006- 2009 | 2010- 2013 | 2014- 2016 | Total cases | Ratio % | |
VGB and VGC disease job | 50 | 61 | 32 | 135 | 41 | 319 | 80.35 |
Tuberculosis NN | 37 | 6 | 7 | 21 | - | 71 | 17.88 |
Leptospirosis NN | 5 | 1 | 0 | 0 | - | 6 | 1.52 |
HIV infection by ear NN risk | - | - | - | - | 1 | 1 | 0.25 |
Total BNN/ BNNdo VSV | 27,878 | 397 | 1.43 | ||||
Maybe you are interested!
-

 Occupational accident and disease regime in Vietnam Social Insurance Law - 5
Occupational accident and disease regime in Vietnam Social Insurance Law - 5 -
 Current Status of Labor Accident and Occupational Disease Regime and Enforcement in Vietnam
Current Status of Labor Accident and Occupational Disease Regime and Enforcement in Vietnam -
 Assessment of Risk Factors for Occupational Microbial Diseases in Healthcare Workers in Can Tho City;
Assessment of Risk Factors for Occupational Microbial Diseases in Healthcare Workers in Can Tho City; -
 Occupational Accident and Disease Regime in Germany
Occupational Accident and Disease Regime in Germany -
 Current Status of Human Resource Training at the Institute of Occupational Health and Environment
Current Status of Human Resource Training at the Institute of Occupational Health and Environment
In Vietnam, epidemiological data show that HCV infection is less common than HBV. The prevalence of HCV in Vietnam was recently estimated at 2% [76]. While a previous study found the prevalence of anti-HCV antibodies to be 1% in a locality in Northern Vietnam [77].