3.3.3. Long-term results after surgery
3.3.3.1. Local recurrence - in the region
Recurrence rate: Re-examination revealed 12 patients with local-regional recurrence, accounting for 8.2%.
Table 3.36. Recurrence rate over follow-up period
Time
Recurrence
12 months | 24 months | 36 months | 48 months | |
Number of patients | 7 | 8 | 11 | 12 |
Percentage | 4.8 | 5.5 | 7.5 | 8.2 |
Maybe you are interested!
-

 Research on agrobiological characteristics of some apricot varieties and technical measures affecting the growth and flowering of Yen Tu yellow apricot in Hanoi - 22
Research on agrobiological characteristics of some apricot varieties and technical measures affecting the growth and flowering of Yen Tu yellow apricot in Hanoi - 22 -
 Characteristics of Business Activities and Business Management Organization at Small and Medium Enterprises in Vietnam
Characteristics of Business Activities and Business Management Organization at Small and Medium Enterprises in Vietnam -
 Characteristics of Activities During the 1000th Anniversary of Thang Long
Characteristics of Activities During the 1000th Anniversary of Thang Long -
 Summary Table of Characteristics of Similar Studies Around the World
Summary Table of Characteristics of Similar Studies Around the World -
 Some characteristics and risk factors of hearing loss in children from 2 to 5 years old in inner-city kindergartens in Hanoi - 1
Some characteristics and risk factors of hearing loss in children from 2 to 5 years old in inner-city kindergartens in Hanoi - 1
Mean follow-up time: 42.2±10.4 months (6- 72 months)
The mean time to recurrence was 18.8±13.7 months for all surgical methods.
Recurrence by surgical method
Table 3.37. Recurrence by surgical method
Time of recurrence
Surgical method
Number of patients | Time from surgery to recurrence (months) | Standard deviation | p | |
Anterior and anterior resection low (n= 51) | 4 | 13.60 | 13.06 | <0.05 |
Pull-through surgery (n=32) | 4 | 27.54 | 18.43 | |
Miles Surgery (n=63) | 4 | 15.54 | 4.68 | |
Total | 12 | 18.79 | 13.69 |
The local recurrence rates for the three groups of patients with rectal resection, pull-through resection, and Miles resection were 7.8%, 12.5%, and 6.4%, respectively.
The group of patients operated by the pull-through sphincter-preserving method had a longer local-regional recurrence time than other surgical methods with 27.54±18.43 months.
3.3.3.2. Overall survival time
The mean survival time of patients in the study was 29.96±19.65 months.
There were 11 patients who died during the follow-up period, accounting for 7.5%. The overall 5-year survival was 84.2%.
Table 3.38. Survival time according to surgical method
Extra life time
(month)
Surgical method
Quantity | Medium | Standard deviation | p | |
Pre-cut and low pre-cut | 51 | 20.98 | 16.54 | <0.001 |
Pull-through Surgery | 32 | 36.00 | 21.54 | |
Miles Surgery | 63 | 29.96 | 19.65 | |
Total | 146 | 29.96 | 19.65 |
The overall survival time of the group of patients operated by pull-through method (36±21.54 months) was longer than that of the other two groups of patients (p<0.001).
The predicted mean survival time was 67.8 ± 2.1 months.
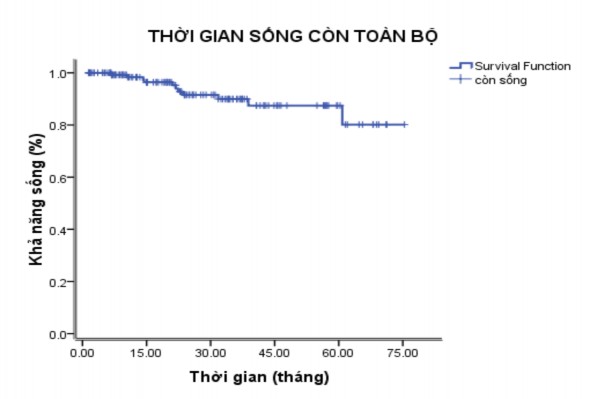
Figure 3.1. Predicted overall survival
3.3.3.3. Disease-free survival time
There were 12 patients with local-regional recurrence during the follow-up period, accounting for 8.2%.
There were 6 patients with distant metastases appearing during the follow-up period, accounting for 4.1%.
Five-year disease-free survival was 80.1%.
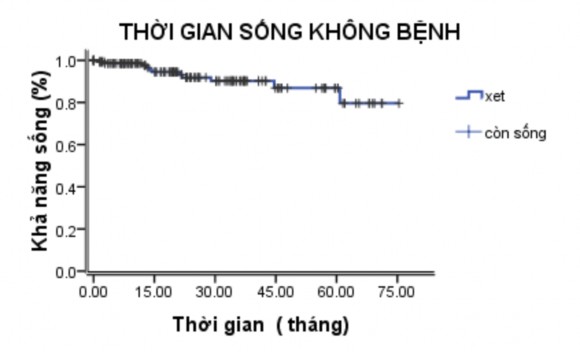
Figure 3.2. Predicted disease-free survival time
3.3.3.4. Quality of life after surgery
Table 3.39. Anal continence function (n = 32)
Kiwan Standard
Number of patients | Percentage | |
I | 15 | 46.9 |
II | 10 | 31.2 |
III | 7 | 21.9 |
Total | 32 | 100 |
Using Kiwan's sphincter function assessment table on patients who underwent sphincter-preserving surgery using the Pull-through method, 25/32 patients (78.1%) had good anal continence results (grades I and II), 7 patients (21.9%) had level III, and no patients had levels IV and V.
Chapter 4 DISCUSSION
4.1. GENERAL CHARACTERISTICS
Through a study of 146 rectal cancer patients treated with laparoscopic surgery, we noted some common characteristics as follows:
Age: Rectal cancer can occur at any age. In our study at Hue Central Hospital, the average age of patients was 59 years old, equivalent to domestic authors such as Vo Tan Long (2003) was 58 years old [44]; Doan Huu Nghi (2003) was 58 years old [61].
The most common age groups in our study were: 41 - 60 (41.8%) and 61-80 (43.8%). In the studies of Doan Huu Nghi and Nguyen Van Hieu, the common age of colorectal cancer in Vietnamese people is 40.
- 60 [33], [47]. In developed countries, the common age is: 40 - 70 years old, because the average life expectancy of these countries is higher. On the other hand, in the research results, we recorded 14 patients, accounting for nearly 10% of rectal cancer patients, under the age of 40, and the youngest patient was only 14 years old. Author Vo Tan Long [44] also had the youngest patient with rectal cancer who was only 17 years old. Rectal cancer is common in the 41-60 age group, which is a worrying fact, when patients in this age group are at an age where they have contributed a lot to their families and society. On the other hand, this is also the age where quality of life is of great concern, so surgical methods that preserve the patient's bowel function are very important.
Gender: The ratio of men and women with the disease in our study was similar (1.08:1), similar to the results of Vo Tan Long [44], Bui Chi Viet [62]. For rectal surgery due to cancer, because the pelvis of men is narrower than that of women, the surgical process will be more difficult, especially
In cases where the tumor size is large, occupying the entire pelvic area, in addition, the surgical anal canal in men is often longer than in women and the enlarged prostate is also the reason why surgery in men is more difficult [39]. However, with laparoscopic surgery, the difficulties due to the above anatomical characteristics have been partly resolved, especially in our study, there were no obese patients with BMI over 30, and nearly 96% of patients had a normal or low BMI (Table 3.4).
4.2. INDICATIONS AND SOME TECHNICAL FEATURES OF ENDOSCOPIC SURGICAL METHODS
4.2.1. Clinical characteristics related to indications
Our research results show (Table 3.5) that up to 40% of patients are hospitalized when their symptoms have lasted for more than 3 months. This proves that many patients are not yet concerned about disorders in the body or because the primary health care situation is still limited. This is also the reason why 88.4% of patients are hospitalized in late stages III and IV, which greatly affects the treatment results (Tables 3.18 and 3.19).
In the early stages, rectal cancer is often discovered by chance or through routine examination, but in the late stages, typical symptoms include fresh blood in the stool, mucus in the stool, changes in bowel habits, and pain and straining during bowel movements.
We noted that bloody stools were the most common symptom that led to hospitalization, accounting for more than 80%. Tables 3.6 and 3.7 show that patients in the study group exhibited all typical clinical symptoms of rectal cancer, such as fresh bloody stools, prolonged bloody mucus stools, and urge to defecate. Of these, the three most common symptoms, in order, were fresh bloody stools, abdominal pain, and bloody mucus stools. In clinical practice, a paradox occurs: when there are no symptoms, diagnosis is often difficult, but
benefits in treatment and high chance of cure; on the contrary, when the patient has full clinical symptoms, it means that the disease is in the late stage, has invaded widely and metastasized far away, so diagnosis is easier, but the chance of radical treatment is low and the cure rate is low, the recurrence rate is high.
To detect rectal cancer in the asymptomatic stage, the best measure is cancer screening. However, to effectively screen for cancer, it is not only the responsibility of the health sector, but also requires close coordination among many sectors: media, health, social insurance, etc. Therefore, up to now, even in developed countries, about 50% of rectal cancer patients are diagnosed late [65]. In our study, 3 patients were diagnosed thanks to colonoscopy due to family factors, even though they had no clinical symptoms. This is also a very useful reminder for clinicians when treating patients with colorectal cancer.
Rectal examination is a very important procedure in diagnosing and providing treatment for patients with rectal cancer, even though modern diagnostic tools have been equipped in large medical facilities such as magnetic resonance imaging or endoscopic ultrasound. Although high rectal tumors were only found in 23 patients, when they were first admitted to the hospital, up to 64 patients did not feel rectal tumors, especially up to 15 patients did not have rectal examination because they had had a previous endoscopy (Table 3.8), raising questions about the clinical skills of the physician. Rectal examination not only determines the presence of cancer, but more importantly, determines the location of the tumor relative to the anal verge [33]. Rectal examination to determine the location of the tumor is sometimes more practical than rectal examination, especially when the tumor is mobile, falling down due to gravity, so when the endoscopy shows the tumor is low, but in fact, the tumor is in a higher position. This can be seen when comparing the results of tables 3.10 and 3.15 of the study. Rectal examination should be performed in the supine position to avoid missing mobile masses.
rectal examination can also assess the extent of tumor invasion, an important criterion for planning surgical methods and prognosis [14].
4.2.2. Paraclinical characteristics related to indications
In addition to clinical symptoms and rectal examination, more objective tests such as colonoscopy with tumor biopsy, computed tomography, abdominal ultrasound, and conventional chest X-ray play a very important role in the diagnosis and treatment of rectal cancer. Although in the conditions of our research facility, magnetic resonance imaging and endoscopic ultrasound have only recently been used, clinical examination combined with rectal examination during surgery, along with endoscopy and 64-slice computed tomography, have allowed us to diagnose and provide appropriate treatment for patients with rectal cancer. Performing colonoscopy in all patients found cancers in different locations, measuring the size from the anal verge to the tumor is the most common and effective way to initially assess the pathological condition [40]. On the other hand, colonoscopy images are more objective and can differentiate between cancers in the rectum and cancers from outside pressing on the rectum. The study results showed that endoscopy detected and biopsied positive in 100% of rectal cancer patients, however, there was a difference in the assessment of tumor location, especially tumors in the intermediate and high segments when compared with rectal examination (Tables 3.9 and 3.14). Postoperative results showed that 64 patients (43.8%) had tumors in the low rectum, 59 cases in the intermediate rectum (40.4%) and 23 in the high rectum (15.8%). Regarding tumor size, 3% of our patients had tumors less than 1/4 of the rectal circumference and more than 65% of patients had tumors occupying more than 1/2 of the rectal circumference.
Tumor location relative to the anal verge is an important criterion in determining surgical treatment for rectal tumors. Combined digital rectal examination