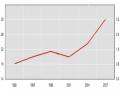
According to Tran Van Chuong (2002) studying 115 patients with pre-training assessment results, the level of complete independence in daily activities accounted for 1.7%, the level of complete dependence accounted for 86.1%.
Author | Completely independent |
Korv J et al (1999) | 38% |
Gresham GE et al (1980) | 35.1% |
Nguyen Thi Nga (2002) | 3.4% |
Tran Thi My Luat (2008) | 1.6% |
Maybe you are interested!
-

 Foreign Studies on Improving Competitiveness for Tourism Development
Foreign Studies on Improving Competitiveness for Tourism Development -
 Comparison of Distribution by Number of Cesarean Sections Between Studies
Comparison of Distribution by Number of Cesarean Sections Between Studies -
 Studies on the Application of Balanced Scorecard in Strategic Management at Foreign Enterprises
Studies on the Application of Balanced Scorecard in Strategic Management at Foreign Enterprises -
 Model of Some Related Studies.
Model of Some Related Studies. -
 Using Cross Currency Contracts to Speculate on the Foreign Exchange Market:
Using Cross Currency Contracts to Speculate on the Foreign Exchange Market:
Table 4.2. Comparison of some foreign studies without PHCN programs
Schutte T et al. [66] reported that 38% of TBMMN patients were completely independent when discharged from hospital, 18% needed assistance and up to 44.5% were completely dependent in daily activities.
The results of our assessment of the independence level of patients before training were lower than those of foreign authors because of better economic conditions and medical development abroad. These people received rehabilitation treatment at facilities with better rehabilitation equipment than in our country and recovered soon after suffering a stroke.
4.2.2. Results of patient's walking recovery
The walking ability of hemiplegic patients due to TBMMN after training using the Bobath method through the study was not much different from the research results of some other authors, with 57.8% of patients being able to walk after 6 weeks of training (Table 3.10).
However, if we compare the results of walking with other authors, our results are still lower. Most of the patients with hemiplegia after stroke mainly use the non-paralyzed leg and the left half of the body.
compensation for the paralyzed side to walk, participation of the paralyzed side in movement
go limited

Table 4.3. Ability to walk independently of hemiplegic patients
Author
Completely independent | |
Jorgensen (1999) | 65% |
Flick (1999) | 78% |
Nguyen Thi Nga (2002) | 60.3% |
Tran Thi My Luat (2008) | 57.8% |


4.2.3. Results of general mobility recovery


Table 4.4. Comparison of general motor recovery results
Author
Do it yourself | |
Benaim (1996) | 70% |
Blanco (1999) | 81% |
Gresham (1999) | 80% |
Nguyen Thi Nga (2002) | 60% |
Tran Thi My Luat (2008) | 69% |


The results of our study on the general motor recovery ability of hemiplegic patients due to TBMMN in tables (3.8), (3.9) show that the rate of patients who are independent in movement after rehabilitation training is lower than the results of studies by some other authors. We believe that such results are reasonable because the rehabilitation specialty in our country developed late and received little attention, and has only recently been applied and expanded in the treatment of patients after TBMMN. The combination of the late development of the specialty, poor equipment conditions and awareness
In the matter of early rehabilitation treatment of patients, there are still limitations. On the other hand, partly because the professional level and training skills of our technicians are lower than those of other countries that have been specialized, all of these factors have affected the treatment results.
4.2.4. Results of recovery of daily living activities
Table 4.5. Comparison of results on independence in daily living
Author
Completely independent | |
Clarke (1995) | 48% - 58% |
Flick (1997) | 45% - 67% |
Gresham (1999) | 69% |
Nguyen Thi Nga (2002) | 16% - 65% |
Tran Thi My Luat (2008) | 13% - 66% |
Our research results on the independence of patients in daily activities in table (3.11) are lower than those of other authors. After training, patients' independence in daily activities is lower than other functional activities. Such results are because we currently do not have occupational therapists in the 6-week period. Patients are mainly trained in movement and walking, and there is almost no training for patients in self-care activities.
4.3. Factors related to recovery outcomes of patients with hemiplegia due to cerebrovascular accident
There are many factors related to the motor recovery results of hemiplegia patients due to stroke. The prognosis and assessment of the recovery ability of hemiplegia patients is difficult to determine accurately in the first examinations in the first week after stroke.
Niam and the authors of the 1990s suggested that it was impossible to accurately determine and assess the recovery ability of hemiplegic patients three weeks after stroke, but it was only possible to predict the recovery ability of patients from 2 to 5 weeks after conducting exercise [64].
Talking about factors related to the recovery results of hemiplegia patients after stroke, many rehabilitation experts have mentioned some of the following basic issues:
4.3.1. Patient's age
Our study results show that patients under 60 years old have better recovery results in both mobility and functional activities in daily life compared to patients over 60 years old (Table 3.12). This result is also consistent with the authors' research results, that is, the younger the age, the better the recovery ability.
According to Cain [59], in people after stroke, the young age group has the ability to recover.
better response to independence in daily living activities than the elderly group.
Although there is no age limit for rehabilitation training for hemiplegia patients due to TBMMN, there are different opinions about the relationship between the age of the patient and their recovery ability. Most authors believe that age is related to the patient's recovery ability, old age is an unfavorable factor in rehabilitation for hemiplegia patients due to TBMMN, the patient's recovery ability decreases as their life expectancy increases [9].
Many recent studies by the authors also conclude that the patient's ability to recover depends on their age. Sween et al. (1996) believe that the patient's age has a great influence on the recovery results.
by assessing the patient's level of independence in movement and daily activities
daily [68].
Blanco (1999) concluded that patients under 70 years of age can recover.
walking ability was 2 times higher than that of patients over 70 years old [52].
With the awareness that the older the age, the more the ability to recover decreases, so some rehabilitation experts have proposed a rehabilitation strategy for young people to practice to restore reduced or lost functions. As for the elderly, the priority is to prioritize compensatory or alternative rehabilitation strategies, to help patients still be able to take care of themselves and be as independent as possible in their daily activities, although the paralyzed person cannot be normalized anymore and in fact normalization is not the main goal of rehabilitation [85].
According to Nakayama H et al., functional progress in daily activities is affected by age. With age, the level of independence in daily activities will decrease compared to youth, the author believes that this is due to the poor recovery ability of the elderly. Every 10 years increase in age will reduce 7% of points on the Barthel scale [61].
According to Schutte T et al. [66], after stroke, the elderly group had a greater level of complete dependence in daily activities than the young group. The authors believe that the reason is that the elderly group has greater functional impairment and risk of recurrent stroke than the young group.
4.3.2. Gender
Many studies have shown the rate of TBMMN in patients.
Male patients are more likely to have a higher rate of relapse than female patients, but the results of rehabilitation between male and female patients are still controversial and not yet completely consistent.
Reynolds et al. (1959) study showed that 18.1% of male patients and 10.7% of female patients had good recovery ability. However, some authors also said that the recovery results between male and female patients were not different [59].
Although the rate of independence in daily activities of men is higher than that of women, this difference is not statistically significant (p > 0.05). There is no correlation between the level of independence in daily activities and the gender of the patient. Thus, it can be said that the results of rehabilitation depend on the patient's self-awareness and willpower, not on gender.
4.3.3. Time to start rehabilitation training.
Research on PHCN has concluded that the best recovery ability of
Hemiplegia due to stroke occurs in the first 3-6 months after stroke.
The World Health Organization (1971) recommended that from the first days after a stroke, even when the patient is still in a coma, prevention of spasticity, contracture deformity and other secondary injuries must be considered as important as prevention of ulcers and other complications in the acute phase. The main technique applied in this phase is the positioning technique. From the first days, the patient is placed in the correct positions according to the recovery model, and the lying positions are changed regularly every 2-3 hours. The correct positioning technique is combined with regular passive exercise of the paralyzed side 2-3 times a day, then depending on the patient's stage of progression, appropriate exercise techniques are applied [47].
Many authors through research on hemiplegia patients show that if patients start rehabilitation training early, the recovery results will be much better than if they start rehabilitation late. However, the authors have not yet reached a consensus.
How early is too early? Many authors believe that patients who start exercising 1-6 weeks after a stroke are in the early stage of rehabilitation.
Andersen (1950) studied 82 patients with TBMMN and found that
Patients who start PHCN training before 3 months will have better results.
compared with patients who started rehabilitation training after 3 months.
Our results shown in Table 3.16 on the relationship between exercise initiation time and recovery results are also consistent with the research results of many authors in the world as well as domestic authors.
Research results show that the earlier the start of exercise training, the better the recovery of general mobility and functional activities in daily life.
4.3.4. Paralyzed side
For patients with hemiplegia due to TBMMN, damage to the right or left cerebral hemisphere will have different clinical manifestations of impairment and reduced ability. In addition to hemiplegia, patients also have other characteristic accompanying disorders.
The rehabilitation results of patients with right hemiplegia and patients with left hemiplegia have been studied by many rehabilitation experts and have given different evaluations.
According to Tran Van Chuong, Nguyen Xuan Nghien, Cao Minh Chau, Vu Bich Hanh, Luong Tuan Khanh and colleagues, the ability to recover movement between patients with left hemiplegia and patients with right hemiplegia is almost not significantly different (right-sided paralysis treated at 75.9%, left-sided paralysis treated at 76.9%) [6].
Differences in right-sided hemiplegia and left-sided hemiplegia
left is still a matter of debate among many authors. Most authors believe that
There is not much difference in the ability to recover between the two sides. If the patient with right hemiplegia is accompanied by aphasia, rehabilitation will be difficult because the patient has difficulty cooperating with the therapist due to the inability to communicate. Meanwhile, the patient with left hemiplegia often has loss of coordination, reduced ability to adjust balance and often has a phenomenon of not accepting the paralyzed side. Thus, rehabilitation of motor function is also very difficult and the ability to recover is not good.
Studies in the 1960s and 1970s by Lorenze and other authors showed that the overall recovery and independence in walking of patients with right hemiplegia and left hemiplegia were no different, but the recovery results of activities of daily living in patients with right hemiplegia were better than those in patients with left hemiplegia [59].
Research on overall recovery outcomes, mobility and walking ability, independence in daily living, disability and disability levels. Handoyo et al. (1994) found no significant differences between left-sided hemiplegia and right-sided hemiplegia patients [57].
Recent studies by authors such as Goldie et al. (1999) also suggest that right or left hemisphere damage causes different clinical manifestations of impairment, reduced ability and disability, but the overall motor recovery results of the two groups of patients are not significantly different [53].
Some other authors believe that patients with left hemiplegia have more severe disorders than patients with right hemiplegia. Basically, the results of general motor recovery of the two groups of patients are not different, but the ability to recover self-care in daily activities in patients with left hemiplegia is worse than that of patients with right hemiplegia [85].
Our research results in table (3.14) show no difference in motor recovery ability between patients with right hemiplegia and left hemiplegia. This result is consistent with the research results of some other authors. Because the body has a compensatory nature, when the right hemiplegia is paralyzed, the left hemiplegia will have compensatory activity adjustment for the right side and vice versa [60], [42].
4.3.5. About the type of brain damage
The ability to recover motor function of hemiplegic patients due to stroke does not depend on the cause of cerebral hemorrhage or cerebral infarction or any other cause. The results in table (3.15) of our study are shown to coincide with many results of other authors' studies.
According to Tran Van Chuong and Nguyen Xuan Nghien, "Initial study of some prognostic factors for motor recovery in hemiplegia patients due to cerebral hemorrhage" showed that the treatment results reached 76.5% due to cerebral hemorrhage, and the treatment results reached 81% due to cerebral infarction.
4.3.6. Paralyzed limb
According to the research results in table (3.17), the motor recovery results between the paralyzed arm and leg are significantly different. The rate of motor recovery in the leg is better (77.4%) than the rate of motor recovery in the arm (40.3%).
According to Tran Van Chuong et al. (1996), the rate of good motor recovery in the legs was 78.2%, and the rate of good motor recovery in the arms was 36.4% [22].
According to Tran Van Chuong and Nguyen Xuan Nghien, the rate of good motor recovery in the legs is 89.3%, in the arms is 57.3% [20].
The reason for the difference in motor recovery results between the arms and legs is still being debated, many authors believe that the right hand performs more complex movements, more sophisticated and skillful movements.
The legs should be more difficult to recover. This is not entirely convincing, because even simple, gross movements of the hands such as shoulder extension, elbow flexion and extension... recover slowly and poorly, not to mention complex movements of the hands and fingers such as wrist flexion, extension, abduction, and contrasting of the fingers with the thumb.
4.3.7. The influence of blood cholesterol on hemiplegia patients
during PHCN treatment
Based on the results of the six-week treatment in tables (3.18), (3.19), we found that the cholesterol content was affected during the training process, with 48 patients (accounting for 77.4%) having a decrease in cholesterol content after treatment. This is consistent with the assessment of many authors, cholesterol content greatly affects patients with high blood pressure, which is a factor that increases the risk of stroke.
According to Le Van Tri, aging increases the aging of arteries due to hardening of the arteries, loss of elasticity, and inability to expand and contract appropriately with blood... therefore, atherosclerosis is a disease of old age [40].
According to Le Van Thinh, Le Duc Hinh, Le Trong Luan, Nguyen Van Chuong (2001), the pathogenesis of stroke is still being discussed both clinically and paraclinically, the rate of hypercholesterolemia in patients with high blood pressure accounts for a high proportion (85%) and this is the main group of risk factors. In our opinion, exercise can be a combined factor to reduce cholesterol for patients.
4.3.8. The effect of Glucose on hemiplegic patients in
PHCN treatment time
In tables (3.16.1), (3.16.2), it is seen that there is no change in glucose content during six weeks of training, which is consistent with the mechanism and pathogenesis of cerebrovascular accident. Blood glucose index depends on the patient's diet and the condition of the pancreas.
CONCLUDE
Through a study on motor function rehabilitation on 62 hemiplegia patients due to stroke based on Bobath's rehabilitation method at the Department of Physical Therapy - Rehabilitation of Thai Nguyen Nursing and Rehabilitation Hospital with a recovery time of 6 weeks, we have the following conclusions:
1. Bobath training is effective in recovery
Function for hemiplegia patients after stroke:
- The patient's ability to sit up after exercise was 77.4% (before exercise was 22.6%).
- After the exercise, 69.3% of patients were able to stand up by themselves (before the exercise, it was 15.1%).
- After the exercise, 57.8% of patients could walk on their own (before the exercise, it was 4.8%).
- After the training, 20.9% of patients were independent in performing functional activities in self-care and daily living (before the training, 1.6%).
2. There are several factors involved in rehabilitation outcomes.
- Patients under 60 years old have better recovery ability in terms of functional activities in daily life.
- Patients who start exercising within 6 weeks after a stroke are more likely to recover.
motor recovery was higher in patients who had exercise after 6 weeks.
-The results of recovering leg mobility in patients with hemiplegia due to stroke were higher than the results of recovering arm mobility in patients with hemiplegia due to stroke.
- For patients with hemiplegia due to stroke after being treated through the acute phase, the Cholesterol index is affected during the process of motor function recovery.
RECOMMENDATION
Through research and discussion, I would like to make the following recommendations:
- It is necessary to examine and diagnose early for patients with hemiplegia due to stroke to have rehabilitation direction for patients as soon as possible.
- Rehabilitation treatment for hemiplegia patients due to stroke by Bobath method is effective. Therefore, in addition to treatment at the hospital, it is necessary to organize training sessions on rehabilitation using Bobath method for hemiplegia patients after stroke to go deep into wards, communes and communities.