The rates of HCV, HBV, and HIV were 76.9%, 65.7%, and 20.5%, respectively, with a duration of use of up to 6 years, and with an injection duration of up to 1 year, the infection rates were 64.7%, 49.8%, and 13.9%, respectively. The results showed that most transmission occurred in the first 6 years and also noted the high infection rate occurring in the first year of injection. According to the results of Vietnam's sentinel surveillance, in 2005-2006, the HIV prevalence was very high among IDUs in Hai Phong (65.5%), Quang Ninh (58.7%), Hanoi (23.4%), Ho Chi Minh City (34.0%), Can Tho (36.6%), and Bac Ninh (21.4%) [31], [4], [34], [25].
IDU is the highest risk group for HCV infection in the world today [75], [149], [53]. Through research on IDU in 57 countries, it was shown that the prevalence of HCV is at least 50% in IDU in 49 countries and territories [84], [40]. In each region, the prevalence of HCV infection in IDU also varies greatly, such as 10-96% in Eastern Europe and Central Asia, 10-100% in South and Southeast Asia, 2-100% in Latin America, 8-90% in North America. In China, Puerto Rico, Russia, Thailand and Vietnam, the estimated prevalence of HCV/HIV co-infection in IDU is up to 90% [84]. A recent study (2010) in Taiwan showed that most IDU are infected with HCV and 99.6% of people infected with HIV-1 are co-infected with HCV [70]. Research on the rate of new HCV infections shows that 90% of new HCV infections in the world are due to IDU (approximately 90% in Australia, 72% in Canada and 54% in the US), 87%-96.9% in Ho Chi Minh City and 31% in Hanoi [100], [21]. HCV is 10 times more likely to be transmitted through needles than HIV. Sharing needles, even just once, can transmit or infect HCV. Harm reduction measures have not been successful with HCV infection. Drug use is certainly more likely to be exposed and each exposure is more likely to transmit HCV than HIV [149]. The risk of infection increases with the duration of injection: 33% of cases have anti-HCV (+) within the first 6 months of IDU and that rate increases rapidly to 62%.
- 90% after 1 year. In general, the majority of chronic infections depend on the status of the HIV infection, especially in developed countries. In Western European countries, the rate of
HCV infection in IDUs varies from 40% to 90% [100], [133]. Factors related to HCV infection rates are gender (male), older age, duration of injection, frequency of sharing needles and having sex with a partner who has IDUs [166]. According to Nguyen Dang Manh (2002), the risk of HCV infection in patients with a history of IDUs is 45.4 times higher than in HCV-infected patients without a history of IDUs [19], [149].
Currently, the prevalence of hepatitis B among IDUs has not been evaluated at the global level. However, research in 59 countries, accounting for about 73% of the world's IDU population, showed that HBV infection rates were highest in countries with high HBV prevalence in the general population (mostly Asian countries). It is estimated that in 2010, there were about 1.2 million (0.3-2.7 million) IDUs infected with HBV, with the largest numbers in Southeast Asia and Eastern Europe [157]. However, hepatitis B vaccine is most widely used for IDUs [53].
1.3.2. Female sex workers (FSW)
According to Guteerrez et al., 2004, a study of 762 female sex workers who immigrated to Spain (75.3% from sub-Saharan countries, 18.2% from South America and 6.4% from Eastern Europe) from 1998-2003 in Madrid. The HIV-1 positive results were 5.2%, HBsAg positive 3.5%, anti-HCV positive 0.8%. HIV-2 and HTLV-II were both unreactive [94]. In Vietnam , according to the results of HIV sentinel surveillance, the HIV/AIDS epidemic has increased rapidly since 1998, especially in the group of IDUs and female sex workers . The rate of female sex workers infected with HIV has increased gradually each year: 2002: 14.5%, 2003: 15%, 2004: 15.5%. In 2005-2006, the rate
HIV infection rates are determined to be very high, such as 29% among street sex workers in Can Tho, and 23% in Hanoi [32]. Drug use among sex workers tends to be increasing and is considered a common phenomenon in Vietnam. IDU behavior is the main risk factor for HIV infection among sex workers [32]. According to a 2000 study by NV Khanh, of over 300 newly arrested sex workers in Loc Ha prison, Hanoi, the rate of drug testing in urine was 38%.
[16]. In a cross-sectional study of 398 street-based female sex workers in Ho Chi Minh City, it was found that: female sex workers who use drugs have a 66 times higher risk of HIV infection than female sex workers who do not use drugs.
Table 1.5 HIV prevalence among PWID in some provinces of Vietnam [32]
City
Year | Study population | Sample size | HIV infection rate | |
Ho Chi Minh | 2000 | PNBD not NCMT PNBD NCMT | 58 53 | 27.6% 67.9% |
Ho Chi Minh | 2003 | PNBD drug addicted PNBD | 381 61 | 11% 44.3% |
Hai Phong | 2004 | PNBD | 215 | 29.8% |
Maybe you are interested!
-
 Experiences of Some Provinces in Laos and Vietnam on Tourism Development
Experiences of Some Provinces in Laos and Vietnam on Tourism Development -
 HIV infection status and care and ARV treatment for children under 18 months of age born to infected mothers in Vietnam, 2010-2013 - 19
HIV infection status and care and ARV treatment for children under 18 months of age born to infected mothers in Vietnam, 2010-2013 - 19 -
 State management of community tourism development in some provinces in the Northwest region, Vietnam - 21
State management of community tourism development in some provinces in the Northwest region, Vietnam - 21 -
 Evaluation of the effectiveness of safe motherhood interventions among mothers with children under 2 years old in 5 provinces of Vietnam during the period 2006 - 2012 - 24
Evaluation of the effectiveness of safe motherhood interventions among mothers with children under 2 years old in 5 provinces of Vietnam during the period 2006 - 2012 - 24 -
 Study on HIV drug resistance in patients receiving first-line ARV treatment in some provinces and cities - 2
Study on HIV drug resistance in patients receiving first-line ARV treatment in some provinces and cities - 2
![HIV Circulation in Some Provinces of Vietnam [32]](https://tailieuthamkhao.com/en/uploads/2025/01/09/hiv-circulation-in-some-provinces-of-vietnam-32-445x306.jpg)
Several studies have shown that prostitution is a high risk factor for HCV infection [19] , [11]. According to a study by ND Manh with 392 PWID, the HCV infection rate was 19.13%. However, this rate in the group of PWID who did not use drugs was 7.18% and in the group of PWID who used drugs was 72.2%. This shows that sexual intercourse transmits HCV less than IDU and sexual intercourse transmits HCV less than HBV and HIV [19].
1.3.3. Multiple blood transfusion patients (MTH)
HIV, HBV, and HCV are the most dangerous of the blood-borne infections and are a global health burden [51]. Because the residual risk of a transmissible infection per unit of donated blood is equal to the risk per unit of transfused blood, the risk of infection increases with the number of units of blood transfused. The risk of undetectable window period viruses, false detection, and immunosilent infections increases the risk of infection in the recipient of a blood transfusion [71], [57]. Screening techniques in developed countries allow for low risk of infection from multiple blood transfusions. The risk per unit is 1 in 10 million for HIV, 1 in 3 million for HCV, and 1 in 72,000 for HBV in Canada, 1999–2000 [71], [176], [57].
Patients with diseases requiring multiple blood transfusions are at high risk of HCV infection. Hemophilia has an infection rate of up to 87% in Germany, 70% in Spain. In an Italian study of 1000 Thalassemia patients, up to 80% were anti-HCV (+) [87]. HCV infection is the main cause of morbidity and mortality in patients with haemophilia. Death from HCV-related liver disease in hemophilia patients is 17 times higher than death from HCV-related liver disease in the general population. Hemophilia patients co-infected with HCV and HIV are 21 times more likely to develop decompensated liver failure than those infected with HCV alone [199]. In fact, all hemophilia patients who required factor transfusion before 1985, when virus inactivation techniques were not available, were infected with HCV. Approximately 80% of these become chronically infected, with 20% progressing to the end stage (cirrhosis, liver failure, and hepatocellular carcinoma) after 20 years [88], [176]. The risk of HCV infection is due to transfusion of blood products such as coagulation factors and immunoglobulins that are not treated to inactivate the virus. After applying the anti-HCV screening program in blood donors, the risk of HCV infection has decreased significantly. Currently, transfused blood has been screened for anti-HCV using ELISA techniques 2 and 3, the risk of HCV infection after transfusion is still very small: 0.01-0.001% in a unit of transfused blood. Brazil (2005): Cross-sectional study of 353 patients with chronic hepatitis B, the highest rate of HCV infection (16.7%), HIV (1.7%), HBV (0.8%) and co-infection 1.7%. HCV infection still has the highest prevalence in this population. High rates of HCV were detected in hemophiliacs (56.6%) and BNCTNT (61.5%). HBV is common in BNCTNT. HIV is mainly found in hemophiliacs [199], [200]. According to Nguyen Dang Manh, in a study of 82 BNTMNL, the rate of HCV infection was 10.97%. The rate of hepatitis C after blood transfusion in the group receiving blood transfusion with anti-HCV screening was lower than that in the group not screened (1.75% vs. 32.0%, p<0.01). The rate of 1.75% HCV infection after HCV screening suggests a risk of transmission through the window period, or poor technique, or possibly
transmission occurs at other stages of the treatment process [19]. Despite improvements in screening techniques, HBV infection remains a high risk for transmission through blood transfusion. This risk is associated with the window period, with latent hepatitis B [67]. However, hepatitis B vaccine is an effective means of prevention for people at risk of infection.
1.3.4. Hemodialysis patients (HDP)
Viral hepatitis and HIV infections are important causes of morbidity and mortality in dialysis patients. Among the viruses that cause hepatitis, HBV and HCV are the most important pathogens in most patients [181] , [173], [151] , [120], [160], [111], [58], [97], [217]. During hemodialysis, both patients and staff are at high risk of hepatitis B infection. HBV prevalence in the dialysis population in developed countries is usually low (less than 10%) but is often higher in developing countries (2% to over 20%) [112]. Up to 60% of dialysis patients infected with HBV will develop chronic hepatitis. However, HBV infection is less prevalent than HCV infection in hemodialysis units. This may be due to the use of hepatitis B vaccine, isolation of HBV-positive patients, and regular surveillance [173].
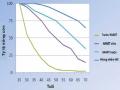
HCV is an important cause of morbidity and mortality in patients with end-stage renal disease [127]. HCV prevalence in end-stage renal disease is high and varies from 2% to 60% across countries and from dialysis units within a country [173], [98], [110]. Although increased attention and regular screening have contributed to a significant reduction, it remains high, with prevalence ranging from 8% to 10% in most developed countries [166]. Prevalence in developed countries ranges from 3% to 31% and above 50% in some developing countries [93] , [83], [79], [221].
Figure 1.4 HCV infection in Asia-Pacific HCWs [111]
Risk factors for HCV infection increase with the number of blood transfusions, dialysis duration, dialysis type, HCV prevalence in the dialysis unit, previous organ transplantation, presence of IDU, male sex, patient age, etc. [166] , [112]. HCV has many opportunities for cross-transmission between infected and uninfected patients in hemodialysis centers [68]. Therefore, hemodialysis at home has a lower rate of HCV infection (8%) than that performed in the hospital (25%). CDC (USA) recommendations, measures to disinfect instruments after each patient have reduced the risk of HCV transmission in hemodialysis units. However, cross-infection occurs at any stage during the implementation process still needs to be monitored regularly for further research.
HBV and HCV coinfection leads to more aggressive liver disease. However, there are few studies on HBV and HCV coinfection in hemodialysis units. According to author GA Reddy (2005), the rate of HBV and HCV coinfection in hemodialysis patients was 3.7%, higher than that in non-hemodialysis patients (0.09%) [173], [97]. In Vietnam, HCV infection was not previously addressed, but only bacterial infection was prevented in hemodialysis units. In 1997, the anti-HCV (+) test at the Hemodialysis Department of Bach Mai Hospital was 82.2%. Since then, measures to prevent cross-infection have been applied, and by 2002, the anti-HCV (+) rate had decreased to 57% [18]. Risk of HCV infection in patients
The risk of infection in patients with periodic hemodialysis with blood transfusion (anti-HCV (+): 67.9%) was higher than that in patients without blood transfusion (anti-HCV (+): 13.3%) (OR: 13.8 (6.2-30.4), p<0.001) [18].
The prevalence of HIV infection in the BNCTNT population varies by country and geographical region. Antiretroviral therapy is the mainstay of HIV prevention in patients with end-stage renal disease [181].
1.4. Measures to prevent HIV, HBV, HCV infection
Strategies for preventing HIV, HBV, HCV infection; especially in cases of HIV coinfection with HCV, HBV viruses, include: Hepatitis B vaccination, education about condoms and safe sex, harm reduction for IDUs. Practice of blood filtration and blood products, safe medical procedures [59], [60], [61], [113]. Antiviral drugs have been used effectively in the treatment of HIV as well as HBV, HCV infection [59], [60], [74]. However, when choosing an antiviral treatment regimen, it is necessary to consider, especially in high-risk subjects. All antiviral drugs have the potential risk of acute or chronic liver toxicity. This risk increases 2- to 3-fold when there is also chronic liver disease such as HBV and HCV. The risk of liver toxicity can be reduced or disappear if hepatitis is successfully treated [59], [60]. Therefore, it is recommended that all HIV-positive patients should be screened for HBV and HCV and vaccinated against hepatitis B. Treatment of HBV and HCV should be considered before treating HIV-coinfected patients [30], [64].
- HIV prevention: According to WHO, effective HIV prevention must include close coordination and concurrent implementation of different strategies: Safe blood transfusion, condom use and safe sex, HIV counseling and testing, harm reduction programs, prevention of mother-to-child transmission, infection control measures in health facilities, management and treatment of STDs. Strengthening preventive measures for target groups
High-risk groups include people with HIV/AIDS, women who have sex with men and their clients, homosexuals, people who receive regular blood and blood products, patients on dialysis, etc.[13], [28].
- Prevention of HBV infection: There are 3 main strategies: One is to change
behavioral, two is passive immunity and three is active immunity:
- Behavioral change: Safe sexual behavior and condom use, infection control measures and improved blood screening measures to reduce the risk of transmission. Condoms are effective in preventing STDs such as HIV, HCV and especially HBV. It can reduce the prevalence of HBV by up to 40% and serological evidence of HBV by 66% in studies of FSWs in high-endemic countries. Therefore, education on behavior change and safe sex is very important [60], [61]. Behavioral change is considered to be more beneficial in developed countries than in developing countries, where infants and young children are at greatest risk of infection. In developing countries, both passive and active immunoprophylaxis are very effective.
- Passive immunoprophylaxis: Used in four cases: Children born to mothers infected with HBV, two is exposure to used needles, three is sexual exposure and four is after liver transplantation.
- Active immunization: Vaccination is the most important strategy to reduce the risk of chronic HBV infection and its complications [81]. Since 1991, WHO has recommended hepatitis B vaccination as a national immunization system in countries with a prevalence of 8% or more and in all countries since 1997. By 2002, 154 countries had routine hepatitis B vaccination programs [187], [106], [107]. By 2008, WHO had expanded hepatitis B vaccination programs to 177 countries with 69% of children receiving 3 doses of vaccine [89], [81], [178]. These strategies are to prevent new infections. The pathological consequences of chronic HBV infection are also prevented by antiviral treatment [107], [89]. Although