2.9%[136], [121]. In these studies, HIV drug resistance mutations occurred mainly in the NRTI group, ranging from 1.1% to 4.5% during 2001–2007 and from 4.8% to 6.5% during 2008–2009. The rate of HIV drug resistance in the PI group was found to be less than 2%. Among the NRTI group mutations, the most common mutations were M184I/V and TAM mutations including M41L, D67N, K70R, T215F, L210W, and K219E/Q (5 studies). The 3 most common mutations in the NNRTI group were Y181 C (6 studies), K103N (5 studies), and G190A (5 studies). For the PI group, M46I/I was more common than other PI mutations (3 studies).
Several studies on HIV drug resistance in patients failing first-line ARV treatment regimens were conducted in Vietnam during the period 2006-2010. In several studies conducted in Ho Chi Minh City from 2007-2009, the rate of HIV drug resistance in the group of patients failing treatment in Ho Chi Minh City ranged from 49% - 55% in adults and 50% in children [47], [93], [16], [22],. In these populations, the rate of HIV drug resistance to NRTI drugs ranged from 47% - 87% and to NNRTI drugs ranged from 37% - 78%. In particular, the rate of resistance to PI drugs was low (<5%). The distribution of HIV drug resistance mutations in this study was 33% - 35% for TAM mutations, 32% - 48% for M184I/V mutations. For the NNRTI group, K103N, Y181C/I/V, G190A/S and Y188L were the commonly observed mutations in this study.
A cohort study to monitor the occurrence of HIVKT in the population receiving ARV treatment and without HIVKT mutations was conducted at the Central Hospital for Tropical Diseases from 2007 to 2009 [18], [19], [20], [21]. In this study, all patients receiving first-line ARV treatment had their HIV viral load measured. Cases with HIV viral load above 1000 copies/ml were sequenced and HIVKT gene mutations were identified. Cases with HIV viral load below 1000 copies/ml were continuously monitored for 24 months to assess the occurrence of HIVKT. The results showed that the rate of HIVKT in patients receiving ARV treatment was 15.2%, of which resistance to the NRTI and NNRTI groups was 15.2% and resistance to the PI group was 0.7%. In
In the group on ARV treatment but with suppressed HIV viral load, the cumulative incidence of resistance mutations in the NRTI group after 24 months was 6.6%, in the NNRTI group was 7%, and in the PI group was 0%.
Several studies on HIV drug resistance transmission have also been conducted in Hanoi and Ho Chi Minh City. The purpose of this study was to assess the status of HIV infection due to transmission, that is, HIV-infected people infected with a previously drug-resistant HIV strain. The study population was young HIV-infected people under 22 years old, first detected with HIV infection and never treated with ARV. In a study conducted in Hanoi in 2006, the rate of HIV drug resistance transmission in this population was <5% [75], which was considered low [116] for all NRTI and NNRTI drug groups. According to a study conducted in 6 HIV testing and counseling rooms in Ho Chi Minh City in 2007 - 2008, the rate of HIV drug resistance transmission was <5%, at a low level [44].
There are several limitations in the surveillance of acquired HIV drug resistance in patients on ART in the studies mentioned above. Cross-sectional studies do not allow assessment of HIV drug resistance mutations at the time of treatment initiation, do not assess the history of ART treatment of patients when starting ART, do not assess the status of potential HIV drug resistance including cases lost to follow-up, treatment discontinuation that occurred before the cross-sectional survey was conducted. Cross-sectional surveys also do not assess the status of patients before the time of treatment failure requiring switching to second-line regimens as well as factors affecting the possibility of the emergence of HIV drug resistance in patients.
The rationale for the 12-month HIVKT follow-up period is that although 3-6 months is sufficient to assess the effectiveness of an ARV regimen, it is not sufficient to assess the effectiveness of an ARV treatment program [57]. Evaluation of the effectiveness of an ARV treatment program also takes into account how the program ensures patient retention in treatment facilities and the provision of treatment services.
ARV continuously. Loss to follow-up, poor adherence to treatment
The disease usually occurs after 6 months of ARV treatment [57].
In Vietnam, there is currently no analysis of the current status of HIV drug resistance prevention practices, the status of early warning of HIV at the treatment facility level, nor are there longitudinal studies assessing the status and factors affecting HIV drug resistance in patients on first-line ARV treatment. In the context of expanding ARV treatment as it is now, assessing the status of HIV drug resistance prevention at the facility level and determining the prevalence of HIV drug resistance in the patient population on ARV treatment is essential in developing appropriate guidelines for the strategy to expand access to ARV treatment in Vietnam.
Chapter 2
RESEARCH METHODOLOGY
The study was designed according to the method recommended by the World Health Organization.
Recommendations for HIV drug resistance studies .
2.1. Describe the current status of early warning of HIV drug resistance at treatment facilities
HIV in some provinces and cities 2010 - 2012
2.1.1. Research subjects, locations and time
2.1.1.1. Research subjects
Selection criteria:
- HIV-infected people receiving first-line ARV treatment;
- There is a satisfactory ARV treatment initiation time at the time of collection for each HIV drug resistance early warning indicator.
Exclusion criteria:
- HIV-infected people not on ARV treatment or on second-line ARV treatment regimen.
- The time to start ARV treatment does not match the required time of the patient.
each index in sample collection.
2.1.1.2. Research location and time
Study location: The study was conducted at 42 outpatient clinics (OPCs) treating HIV-infected people in 23 provinces and cities (Appendix 1). The OPCs were selected according to the following criteria:
- Is a facility that has been providing ARV treatment for at least one year or more
- By treatment level: central level, provincial level, district level
- By geography: North, Central and South
Research implementation period: May 2010 to December 2012.
2.1.2. Research method
2.1.2.1. Research design:
The study was designed using a cross-sectional descriptive method.
At the selected research facilities, the research team, together with staff working at HIV/AIDS treatment clinics, selected medical records according to the time frame of each year of data collection for each specific research indicator.
2.1.2.2. Research indicators and time frame for collecting each indicator:
Although WHO recommends collecting 8 early warning indicators of HIV drug resistance, based on the current situation of ARV treatment in Vietnam, after consulting with WHO experts, the research team decided to choose 5 indicators to include in the study, including:
1. Indicator 1: Proportion of patients prescribed ARV treatment regimens according to the guidelines
Ministry of Health guidelines (EWI 1);
2. Indicator 2: Proportion of patients who dropped out of treatment within 12 months of first-line ARV treatment (EWI 2);
3. Indicator 3: Proportion of patients maintaining first-line ARV treatment at 12 months after treatment (EWI 3);
4. Indicator 4: Percentage of patients who return for follow-up visits on time (EWI 4) within 12 months
after first-line ARV treatment;
5. Index 5: Number of months in a year that the treatment facility did not run out of any medication
ARV (EWI 5).
There are 3 early warning indicators of HIV drug resistance recommended by WHO but
The research group decided not to include:
- On-time medication delivery index
- Treatment adherence index by counting the number of remaining pills
- Index of the proportion of patients achieving HIV viral load suppression (<1000 copies/ml) after 12 months of first-line ARV treatment.
The reason for omitting the above three indicators is that in Vietnam, the medication collection schedule often coincides with the follow-up examination schedule. The adherence index by counting the number of ARV pills cannot be performed because the HIV/AIDS treatment process in Vietnam does not include the content of assessing patient adherence to treatment by counting the remaining pills. The index of achieving the HIV viral load suppression threshold cannot be performed because Vietnam does not perform routine HIV viral load testing.
Sample collection timeframe for each research indicator:
For the indicators EWI 1 (prescription according to the first-line ARV regimen recommended by the Ministry of Health), EWI 2 (rate of patients dropping out of treatment), EWI 3 (rate of maintaining the first-line ARV regimen after 12 months of treatment): The time of the selected samples for each year of data collection is specifically as follows:
2010 : group of patients started ARV treatment from January to December 2009. 2011 : group of patients started ARV treatment from January to December 2010. 2012 : group of patients started ARV treatment from January to December 2011.
For EWI 4 indicators (proportion of patients attending follow-up appointments on time): All patients on ARV treatment who attended scheduled appointments in the fourth quarter of the year prior to the year of data collection.
For EWI 5: Continuous drug supply: Number of months in which the treatment facility's warehouse does not run out of any ARV drugs being prescribed to patients, the sample collection time frame is 12 months of the year before the collection year. Specifically, data collection in 2010 collected reports on the use and inventory of ARV drugs in 2009; for the 2011 assessment, reports from 2010 were collected, and for 2012, reports from 2011 were collected. Information was collected from reports on the import and export of ARV drugs at the pharmacy department, the sampling time depended on the year of data collection.
2.1.2.3. Sample size
The formula for calculating sample size for each indicator is performed according to the recommendations of
WHO for the assessment of early warning indicators of HIV drug resistance[103]: N = n 0 / (1 + (n 0 -1)/n); n 0 = Z 2 *p*(1-p) / e 2
In there:
Z = 1.96; p = 0.5 (estimated prevalence of each indicator); e = precision = 0.07 (based on 95% confidence interval with ±7% bias); n = Number of patients on ARV treatment at each treatment facility.
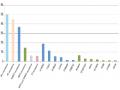
However, based on the reports on the actual treatment situation at the treatment facilities, the research team decided to collect all medical records of eligible patients at the participating facilities for all research indicators. Specifically, the number of medical records collected is presented in Table 2.1.
Table 2.1. Number of medical records and drug inventory reports collected
for each index by year
Indicators
Number of medical records/reports collected each year | ||||
2010 | 2011 | 2012 | ||
EWI 1 | Percentage of patients prescribed the correct regimen according to regulations Ministry of Health | 5.122 | 4,542 | 4,678 |
EWI 2 | Rate of patients dropping out of treatment within 12 months of commencement ARV treatment head | 5,631 | 4,778 | 4,727 |
EWI 3 | Proportion of patients maintaining first-line ARV regimen after 12 months month | 5,631 | 4,778 | 4,727 |
EWI 4 | Rate of patients returning for follow-up visits on time in the quarter | 4.365 | 5.134 | 5,536 |
EWI 5 | Number of months in the year the facility did not run out of any ARV drugs (status report) drug inventory at treatment facility) | 12 | 12 | 12 |
Maybe you are interested!
-

 Current status of HIV infection, AFB + tuberculosis and evaluation of preventive intervention effectiveness among drug addicts in Dak Lak province - 1
Current status of HIV infection, AFB + tuberculosis and evaluation of preventive intervention effectiveness among drug addicts in Dak Lak province - 1 -
 HIV Drug Resistance Surveillance and Prevention Situation in the World
HIV Drug Resistance Surveillance and Prevention Situation in the World -
 Business registration under Vietnam Enterprise Law - Current situation and some recommendations - 1
Business registration under Vietnam Enterprise Law - Current situation and some recommendations - 1 -
 Recruitment of civil servants at the People's Committee of Luc Nam district, Bac Giang province - Current situation and solutions - 9
Recruitment of civil servants at the People's Committee of Luc Nam district, Bac Giang province - Current situation and solutions - 9 -
 Prohibition of discrimination in Vietnamese labor law - Current situation and some recommendations - 2
Prohibition of discrimination in Vietnamese labor law - Current situation and some recommendations - 2
2.1.3.Sample collection:
2.1.3.1 Building and testing the toolkit:
The data collection tool was designed according to the data collection form recommended by WHO in 2009[103]. The forms were tested, revised and agreed upon by the research team members. Before testing the tool, the research participants were trained on how to collect data, problems that may arise during the data collection process and how to resolve them, and research ethics.
The data collection toolkit includes:
- Initial ARV regimen prescription practice form : collects all first ARV regimens prescribed by physicians for patients starting treatment at each facility, excluding patients transferred from other facilities. Information collected includes patient codes and ARV regimens prescribed by physicians (Appendix 2a for adult patients and Appendix 2b for pediatric patients).
- Sample for monitoring the status of patients still alive and patients still on first-line ARV regimen : Information is collected for each group of patients in each treatment month of the data collection year. This information includes the number of patients starting treatment, the number of patients transferred, the number of patients transferred, the number of deaths, the number of patients still alive and on first-line ARV treatment, the number of patients still alive and on second-line ARV treatment, and the number of patients who stopped treatment (Appendix 3).
- Patient dropout form : Records information about patients who do not return for follow-up visits for more than 3 months. Information collected includes patient code, treatment start date, date of last visit and date of last appointment. Information about reasons for dropout and date of return for treatment, if any, is also collected (Appendix 4).
- Sample of on-time follow-up visit : Information collected includes patient code, date of visit and date of follow-up visit of original visit (take the visit in the month).