LIST OF TABLES
Table 2.1. Sample distribution 37
Table 3.1. Distribution of disability types of children with disabilities before and after intervention 48
Table 3.2. General information about mothers with children aged 0 - 12 months 49
Table 3.3. Average age of children through stages of early detection of disabilities by month50 Table 3.4. Average age of children through stages of PHSKT and time from first detection of DHBT to definitive diagnosis by type of disability51
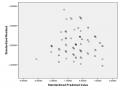
Table 3.5. Multivariate regression model to determine factors related to the time of first detection of DHBT 52
Table 3.6. Multivariate regression model identifying factors associated with the time when children were diagnosed with disabilities 54
Table 3.7. Knowledge about disabilities and disability prevention measures of mothers with children aged 0-12 months before and after intervention 56
Table 3.8. Knowledge of PHSKT of mothers with children aged 0-12 months before and after intervention 56
Table 3.9. Knowledge of signs of autism of mothers with children aged 0 - 12 months before and after intervention 57
Table 3.10. General knowledge of PHSKT of mothers with children aged 0 - 12 months before and after intervention 57
Table 3.11. Views/attitudes towards TKT of mothers with children aged 0 - 12 months in the pre-intervention and post-intervention groups 58
Table 3.12. Concepts/beliefs about the role of mothers in PHSKT of mothers with children aged 0-12 months in the pre-intervention and post-intervention groups 58
Table 3.13. Attitudes towards PHSKT in the community of mothers with children aged 0-12 months in the pre-intervention and post-intervention groups 59
Table 3.14. Attitudes towards participating in PHSKT activities in the community of mothers with children aged 0 - 12 months before and after intervention 59
Table 3.15. General PHSKT attitudes of mothers with children aged 0-12 months before and after intervention 60
Table 3.16. Practices of monitoring child development signs of mothers with children aged 0-12 months before and after intervention 60
Table 3.17. Practice of monitoring signs of gross and fine motor development of mothers with children aged 0-12 months before and after intervention 61
Table 3.18. Practice of monitoring signs of visual impairment in mothers with children aged 0 and over
-12 months old before and after intervention 61
Table 3.19. Practice of monitoring signs of intellectual disability of mothers with children aged 0 - 12 months before and after intervention 62
Table 3.20. Practices of searching and using PHSKT documents of mothers with children aged 0-12 months before and after intervention 62
Table 3.21. General PHSKT practices of mothers with children aged 0-12 months before and after intervention 63
Table 3.22. Average scores of knowledge, attitudes and practices of PHSKT of mothers with children aged 0-12 months before and after intervention 63
Table 3.23. Association between intervention activities and knowledge, attitudes and practices of PHSKT of mothers with children aged 0 – 12 months 64
Table 3.24. Average age of early detection stages before and after intervention 66
Table 3.25. Average age in months of early detection stages before and after intervention by type of disability 67
Table 3.26. Average age in months from first detection of DHBT to diagnosis before and after intervention by type of disability 68
LIST OF CHARTS
Chart 3.1. Average age of disabled children by month 47 years old
Figure 3.2. Gender distribution and birth order of children with disabilities before and after intervention 47
Figure 3.3. Distribution of disabilities in children and causes of disabilities 48
Figure 3.4. Distribution of mothers with disabilities receiving PHSKT information (n=220) 49
Figure 3.5. Distribution of TKT examined and diagnosed before screening (n=220) 50
LIST OF IMAGES
Figure 1.1. Model to enhance early detection of disabilities for mothers with children under 6 years old in Hoai Duc district - Hanoi city 23
Figure 1.2. Information, motivation, and behavioral skills model 25
Figure 1.3. Administrative map of Hoai Duc district - Hanoi city 30
Figure 2.1. Research design diagram 33
Figure 2.2. Theoretical framework for applying the IMB model in enhancing early detection of defects 44
LIST OF ABBREVIATIONS
Ages & Stages Questionaires | |
BHBT | Abnormal manifestations |
Labor, War Invalids and Social Affairs | Labor, War Invalids and Social Affairs |
Medical staff | Health Officer |
CTS | Early intervention |
DHBT | Abnormal signs |
GVMN | Preschool teacher |
ICF | In ternational Classification of Functioning Disability and Health (International Classification of Functioning, Disability and Health) |
IMB | Information, Motivation and Behavioral Skills Model (Mo information, encouragement, behavioral skills) |
KAP | Knowledge Attitude Practical |
KT | Disability |
M-CHAT | Modifier – Checklist Autism in Toddle Modified Childhood Illness |
NCS | PhD student |
NKT | People with disabilities |
PHS | Early detection |
PHSKT | Early detection of defects |
PHS – CTS | Early detection - early intervention |
PHCN | Rehabilitation |
PHCNDVCĐ | Community-based rehabilitation |
Decision of the Ministry of Health | Decision – Ministry of Health |
QH | National Assembly |
TB | Medium |
TDHV | Education level |
TQS | Ten Questions Screen |
Maybe you are interested!
-
 Assessing the Impact of Quality of Work Life on Work Performance – Model 1 - Impact of Quality of Work Life
Assessing the Impact of Quality of Work Life on Work Performance – Model 1 - Impact of Quality of Work Life -
 Research Model and Research Methodology to Analyze the Impact of Bad Debt on Bank Efficiency
Research Model and Research Methodology to Analyze the Impact of Bad Debt on Bank Efficiency -
 Assessing the Impact of FDI Capital Flows on the Socio-Economic Development of Quang Ninh
Assessing the Impact of FDI Capital Flows on the Socio-Economic Development of Quang Ninh -
 Assessing the impact of social capital on the operations of commercial banks in Ho Chi Minh City - 21
Assessing the impact of social capital on the operations of commercial banks in Ho Chi Minh City - 21 -
 Goffi G's Model for Assessing Tourism Destination Competitiveness and Sustainability
Goffi G's Model for Assessing Tourism Destination Competitiveness and Sustainability
Children with disabilities | |
TP | City |
Medical Center | Medical Center |
TYT | Medical Station |
Secondary School | Junior High School |
High School | High school |
SSC | Standard error |
UNESCO | United Nations Educational Scientific and Cultural Organization (United Nations Educational, Scientific and Cultural Organization) |
UNFPA | United Nations Population Fund (United Nations Population Fund) |
UNICEF | United Nations Children's Fund |
WHO | World Health Organization (WHO) |
PROBLEM STATEMENT
Childhood is a critical period of growth and development because experiences during this period can influence an individual's entire life [92], [109]. For children with disabilities (CDs), early detection (ID) and early intervention (II) during this period are very important because they help them maximize their potential and create opportunities for them to integrate into society, reducing the burden on their families and society [109], [139]. A type of disability plays an important role not only in establishing a CTS program but also in determining the success of a CTS program for that type of disability [74]. However, up to half of children with disabilities are not identified before going to school. This causes children to lose the opportunity to receive CTS and increases the cost to society in the later intervention process [119]. According to Shonkoff, if children with disabilities are detected and intervened before kindergarten, society can save from $30,000 to $100,000 per child with disabilities [139].
In developed countries, early detection of disabilities (ED) in children is a fundamental part of child health care [87]. This activity is often integrated into the activities of health systems, education and other social care services [84]. In low- and middle-income countries, the implementation of EID has not received due attention and its implementation remains a major challenge [80], [135].
In Vietnam, one of the first programs with PHSKT content for children is the community-based rehabilitation program (PHCNDVCĐ). Besides the PHCNDVCĐ program, there are also a number of PHSKT projects for children implemented by the government, non-governmental organizations and individuals, but according to the assessment of the Ministry of Health, this activity is still underdeveloped [9].
PHSKT is the responsibility of the whole community, including the responsibility of the family [8], [9]. In the family, mothers are the closest to children, they often observe and pay attention to children's development and they tend to compare their children with other people's children to form assessments or they compare development from simple cognitions and behaviors to complex thinking skills [88]. They themselves seek and use information about development at the most basic level [129]. There have been many studies
Studies have shown that mothers are early in recognizing developmental abnormalities (DAD) in their children and that maternal concerns about their children's development are as sensitive and specific as quality screening tools. These studies have also shown that maternal concerns about their children's development and behavior are directly related to screening results for developmental and behavioral problems [90], [91].
Glascoe pointed out the advantages of PHSKT through mothers such as: The cooperation of mothers with medical staff is significantly improved, when mothers detect abnormal signs in their children, the time for diagnosis is significantly shortened. PHSKT in children through mothers eliminates challenges such as children not cooperating, afraid, sleepy or sick... when medical professionals directly measure the skills of children. PHSKT through mothers has significantly improved the rate of early detection of children with autism [95] . However, many international surveys have shown that many parents need advice on methods to detect DHBTs in child development [47], [72].
In Vietnam, there have been only a few studies on knowledge, attitudes and practices of PHSKT in children on the group of parents of children with disabilities [4], [38]. These studies have shown that most parents of children with disabilities lack knowledge about their children's psychophysiological development, lack knowledge and skills to detect types of disabilities (KT) related to the brain such as intellectual disability, behavioral disorders and especially cerebral palsy, so they did not promptly detect signs of developmental delay in their children [4], [26], [38].
In Hoai Duc district - Hanoi, the PHCNDVCB program is managed by the Public Health Department of the health center (TTYT). However, the program's current activities only stop at synthesizing and reporting data. According to statistics from the TTYT, Hoai Duc district has 3,138 people with disabilities (PWD) but there is no data on PWD under 6 years old. In Hoai Duc district, there has not been any research on knowledge, attitudes and practices of PHSKT in children of mothers [35].
To study the current status of PHSKT in children and initially evaluate the impact of interventions to enhance PHSKT in children for mothers in Hoai Duc district, we conducted a study "Evaluating the impact of the model to enhance early detection of disabilities for mothers with children under 6 years old in Hoai Duc district - Hanoi city in the period 2014 - 2016" .