CSNB documents in medical records include: vital function monitoring form, nurse form and some other forms according to Decision No. 4069/QD-BYT dated September 28, 2001 on promulgating medical record forms of the Ministry of Health and according to the specialized nature as prescribed by the hospital. CSNB documents in medical records must ensure the following requirements [ 23 ] :
- Record patient information accurately and objectively.
- Unify information on patient care work of nurses, midwives and treating physicians. Differences in assessment, monitoring and evaluation of patient condition must be promptly discussed and agreed upon between those directly caring for and treating the patient;
- Record fully and promptly the disease progression and nursing interventions.
Maybe you are interested!
-

 Current Status of Self-Assessment of Classroom Management Competency
Current Status of Self-Assessment of Classroom Management Competency -
 Managing medical ethics education for nursing students in medical colleges - 32
Managing medical ethics education for nursing students in medical colleges - 32 -
 Assessment of the Quality of Sustainable Tourism Development Factors in Nghe An Province from Provincial Tourism Management Officers
Assessment of the Quality of Sustainable Tourism Development Factors in Nghe An Province from Provincial Tourism Management Officers -
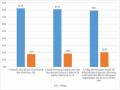
 Respondents' Assessment of Operational Risk Management at Agribank Quang Tri Province Branch
Respondents' Assessment of Operational Risk Management at Agribank Quang Tri Province Branch -
 Perfecting the Organization of Applying the Production Cost Accounting Method to Serve Cost Management Accounting
Perfecting the Organization of Applying the Production Cost Accounting Method to Serve Cost Management Accounting
Medical records must be stored according to the provisions of Clause 3, Article 59 of the Law.
Medical examination and treatment.
Managing patient records is a very important task for health workers in general and for the EDT in particular. From the stage of receiving hospital records to managing the recording, storage, preservation and summary of records. The EDT must ensure that the records are clear, accurate, complete and legal.
1.4.2 Method of assessing nursing management capacity:
- Periodic, regular assessment : Is a regular assessment by the manager. This form of assessment is often used by managers on a daily, weekly, monthly basis to urge and monitor subordinates to perform well their personal and unit tasks. Superior managers often apply quarterly, semi-annual, and annual assessment forms. Regular assessment standards are issued and announced in advance for the unit to self-review and self-assess. Superiors who come to assess subordinates can use the assessment results of the unit and only review some necessary points or re-assess the entire assessment according to the previously announced assessment standards.
- Ad hoc assessment : Is an assessment that is not announced in advance. This form of assessment often focuses on a specific topic, is objective and effective, but does not cover all the work of the unit or individual.
This form of assessment often encounters resistance from individuals and units being assessed if the assessor is unprofessional, the assessment criteria are unclear or not built on standards that have been communicated to the unit.
- Intermittent and ad hoc periodic evaluation : The evaluation unit notifies the evaluation content and criteria in advance but does not notify the evaluated unit of the specific evaluation time in advance. This form of evaluation combines both of the above forms, creating an open atmosphere for the evaluation [ 6], [10], [11], [39], [95].
1.4.3 Factors affecting nursing management capacity : Factors affecting nursing capacity include:
- Nursing qualifications are still low, the rate of nurses graduating from college or university is below 10% and the rate of skilled nurses is > 80%, leading to proactive care, the ability to assess and make independent decisions in care, leading to limited efficiency and quality of nursing care [127], [129] .
- Nursing administrative work and paperwork take up a proportion of time equivalent to direct nursing staff time (28%). Because currently, most of our hospitals are mainly using books and traditional recording methods, hospital fee payment procedures in departments are also a burden for nurses, they have to spend too much time on administrative procedures due to the lack of a medical secretary system. Meanwhile, each activity and task does not have a manual or workflow to help with systematic and unified management [ 94 ] .
- The awareness of staff, self-esteem and complacency of medical staff about nurses also partly affect the management activities and the coverage and expansion of CSNBTD in hospitals.
- Doctor's hegemony: This is an important factor because in the past as well as the present, doctors are still the ones who make decisions, so they do not want nurses to develop more strongly, because if nurses are trained in basic skills, the role of doctors will be reduced, the monopoly position will be lost, having someone to supervise activities will increase quality and efficiency.
- Coordination between nurses and nurses: It is found that senior nurses with positions in the organization do not want young people to have the opportunity to develop because then it is easy to change their position in an organization and these people often have close relationships with doctors to have more opportunities and a voice. Therefore, enhancing coordination with colleagues and discussing plans, methods, and content will bring high efficiency in management and CSNB [ 79 ] .
- Nurses often have passive and dependent behavior, they do not actively participate in the fight for the industry. They just wait for some people to do it for them. Leaders at all levels who care and encourage will help care work to be proactive and promote creativity.
- And the fighting between the directors in the same agency makes the internal
The industry is often not united...
- Lack of opportunities for education and retraining in expertise and management: this is the reality in Vietnam, most nursing schools are led by doctors, school leaders do not want to create conditions and still have limited views. Many qualified nursing students are eager to learn and want to improve their qualifications, but in Vietnam, only Ho Chi Minh City University of Medicine and Pharmacy offers postgraduate training, so it is difficult to apply for further study [ 22], [69 ] .
- In addition, low income, large number of patients, lack of equipment and poor coordination between patients and their families are also factors that significantly affect the quality of nursing work [ 10], [41 ], [107] .
1.5 Nursing Competency Research :
1.5.1 In the world :
Many studies on nursing capacity [33] , [117] in the world show that: Nurses with skills play a very important role in the success of health care organizations, are the central factor in the interaction between patients, nurses, doctors, technicians, other staff and hospital leaders. Nurses are advocates for patients and their families, and they play a core role in ensuring patient safety and quality of care. In addition, they are responsible for managing human resources, resources, equipment and financial management [116], [119] .
Today, the role of the nurse is considered one of the most difficult and complex roles in the health system. This view is also similar to the research of Chase (1994), who studied the capacity of the nurse, she said that "The head nurse has an important management role because they have a great influence on the success of the health organization". Besides, Sanders, Davidson, and Price (1996) pointed out that the nurse is the one who conveys the goals, orientation, and criteria of the health organization (hospital, department, ward, nursing center) from the management perspective to clinical practice; therefore, the position of the nurse requires the ability to communicate general guidelines and integrate them into management and clinical practice while simultaneously defining and managing outputs. The role of the DT is extremely important because they are the ones who connect the orientation, goals, and missions of the organization with the people who provide daily care for patients. In addition, the DTK is not only responsible for management but also responsible for the CSNB activities in the department throughout the 24 hours.
To form and develop capacity for ethnic minorities, in developed countries, they apply many models such as providing formal knowledge from schools, or mentorship programs, conferences, and seminars.
According to AONE (2005), today's DTs are required to have competence in
the following areas [16], [33 ]:
Communication skills and the ability to build and manage relationships: Effective communication, relationship management, influencing behaviors, ability to work with diversity, shared decision making, community involvement, health care worker relationships, academic relationships.
Understanding of the healthcare environment : Clinical practice knowledge, patient care delivery models and work design knowledge, health care economics knowledge, health care policy knowledge, governance knowledge, evidence-based practice knowledge, outcome measurement knowledge and dedication
for patient safety, utilization/case management knowledge, quality improvement and data knowledge, risk management knowledge [153], [156] .
Leadership skills : Basic thinking skills, personal journey discipline, ability to use systems thinking, follow up planning, Thange management.
Professional skills: Personal and professional responsibility, career planning, ethics, evidence-based clinical practice and management, advocacy for clinical enterprise and nursing practice, active membership in professional organizations.
And financial and resource management skills: Understanding of healthcare finance, human resource management and development, strategic management, marketing, information and technology management. Of which, the 3 influencing aspects are:
Personal factors/characteristics; Occupational factors/characteristics ; Between
personal factors/characteristics and organizational characteristics. Other factors ...
In Thailand [ 53 ], the Philippines has specialized nursing training such as geriatrics, pediatrics, and obstetrics. Training ensures quality according to nursing competency standards, including management standards.
Regarding scientific research in nursing, according to Tiran and colleagues at Greenwich University in London, clinical nurses lack time, ability, and motivation to conduct research; lack of leaders to promote and guide research, this is also one of the reasons why clinical nurses do not have or have reduced research capacity [154].
A study on the knowledge, skills, and attitudes of nurses and midwives by Pamela Duffy and colleagues (2008) in the US showed that there was a difference in awareness of evidence-based practice in clinical departments of provincial hospitals before and after training. Regarding skills before training, the rate of nurses and midwives with clinical practice confidence was 46%, after training it was 65% (p = 0.018), and there was a similar difference in attitude (p = 0.046) [140].
According to Roderick's study in the US on improving the quality of healthcare [147] , the rate of patient satisfaction with doctors is higher than that of nurses and midwives in clinical departments.
In the obstetrics department, satisfaction with nurses and midwives was 73% and with doctors was 71%.
If we have adequate research on these aspects, have convincing and objective evidence applied to improving the capacity of DT workers , there will be many positive changes in improving the professional status as well as the quality of CSNB as we have seen more or less about the special role and position of DT workers.
In general, research topics related to the capacity of the DDT in the world focus on the standards of leadership and management capacity, behavioral research, and attitudes towards work and patients. Research on skills and management processes in daily work has not been found or has been limitedly mentioned in some related studies [157], [158], [159] .
1.5.2 In Vietnam :
1.5.2.1 Regarding professional qualifications :
Currently, the professional level of the nursing staff, hospital and department nurses in our country is mostly at the college level, the proportion of those with university and postgraduate degrees is low. Mostly women, the average age is over 40 years old and the majority. The ability to perceive expertise is still passive, mainly relying on medical orders and implementing medical orders, with little thinking, creativity, and innovation in the quality of nursing care [ 34], [35], [57 ] .
Technical procedure steps are often skipped. Some specialized and advanced nursing techniques are not systematically trained in schools [107].
According to the study of Nguyen Thi Thanh Dieu and colleagues: the proportion of female nurses is the majority (71.5%), the age under 30 accounts for the highest proportion (62.8%). The professional level is mainly TC level (94.3%). The survey results show that 100% of patients admitted to the hospital had their pulse, temperature, and blood pressure measured, of which 96.7% were measured immediately after 15 - 30 minutes, 4.2% were measured within 60 minutes. However, the rate of guidance, explanation and taking patients to do tests is still low (81.6%), relying on family (18.4%). This is one of the causes of inconvenience for patients [31] .
Performing the steps in the technical process, Nguyen Thi My Linh's research showed that 75.7% performed correctly, 24.3% did not meet the requirements. Ensuring sterility in invasive procedures was achieved by 74.6%, and not achieved by 25.4%. Only 38% of instructions, advice and health education were done well [ 51 ].
The research team shows that most of the nursing staff are women, which is also consistent with the nature and characteristics of the profession; Intermediate level of expertise still accounts for a high proportion; Performing common nursing technical procedures still skips steps, and specialized techniques are still limited. This situation reflects the current weaknesses of the Vietnamese nursing system in the stages of enrollment, training organization, recruitment and management [50 ] .
Based on some nursing technical procedures to evaluate professional level is one-sided and inaccurate. This is a limitation of the topics, it is necessary to have many information channels such as evaluation from direct managers, patients and the effectiveness of the work that the person being evaluated performs.
Therefore, it is necessary to combine qualitative research with quantitative research to supplement
Additional comments ensure objectivity and accuracy.
1.5.2.2 Regarding nursing management :
The DTs are mainly appointed from the DTs, have not been trained in management, work based on experience, and do not know or do not know enough about LDDD skills. In the management process, many issues have not been correctly identified, priorities are not selected in accordance with resource conditions, so the efficiency is not high, even wasting time, human resources and financial resources. The quality of medical services is still complained by people [ 10], [37], [76 ].
The study by Nguyen Thi Thanh Dieu and colleagues proposed 3 solutions to improve the quality of nursing care: Increase the training target of nursing bachelors to meet basic and specialized knowledge in nursing care. Improve foreign language and information technology skills for nurses to access scientific and technical advances, creating opportunities for exchange, learning and integration in the region and the world. Strengthen the role of nurses in the work of checking and evaluating the quality of care [31 ].
According to the results of the survey on the organizational system and human resources of the Vietnam Nursing Association in 2007, the team of nurses at all levels in hospitals in Vietnam has limited professional qualifications, 90.6% are TC, and 23.9% are under 35 years old. The rate of nurses who have not received management training is still high (62.2%) [ 42 ];
Pham Duc Muc's study [ 59 ], investigating the system and human resources of the central and provincial hospitals in 2007, showed that: the professional level of postgraduate was 1.2%; university was 24.2%; college was 14.9% and college was 59.7%. Regarding the training major of pharmacy: 82.0%; students 7.1%; technicians 4.4% and other 6.5%. Trained in labor management was 63.3%. Regarding age
<35 accounts for 12.1%; 26 - 45 years old accounts for 41.7%; 46 - 55 accounts for 44.6%; >55 years old accounts for 1.6%. Regarding the implementation of duties and responsibilities: Organizing and directing the implementation of CSNBTD: good 72.3%; average (average) 22.1%; poor 4.1%; not done 1.5%. Urging and checking the correct implementation of technical procedures and hospital regulations: good 90.0%; average 3.2%; poor 5.2%; not done 1.5%. Organizing training and improving qualifications: good 62.4%; average 22.5%; poor 9.2%; not done 5.9%. Participating in guiding practice for students: good 35.8%; average 31.4%; poor 26.6%; not done 6.3%. Planning for purchasing, checking usage and preservation: good 48.0%; average 31.4%; poor 26.6%; not done 6.6%. Checking hygiene and anti-infection work: good 88.2%; average 5.5%; poor 5.2%; not done 1.1%. Participating in organization and recruitment work: good 60.5%; average 24.0%; poor 12.5%; not done 3.0%. Participating in scientific research: good 38.0%; average 22.1%; poor 34.7%; not done 5.2%. Participating in line guidance: good 45.8%; average 20.3%; poor 22.8%; not done 5.2%. Periodically reviewing and summarizing: good 62.0%; average 27.5%; poor 8.0%; not done 2.5%. Participate in proposing ideas related to CSĐD: good 77.9%; average 17.0%; poor 4.1%; not doing 1.1%.
According to the study of Do Dinh Xuan (2007) [107], the whole country has 6,787 nurses working in public hospitals nationwide (statistics from 30 central hospitals and 63 Departments of Health), of which: Nurses account for 78.4%, students account for 7.4%, Medical Technicians account for 8.2%, and 6.0% of nurses without specialized qualifications are nurses participating in management of medical staff (physicians, pharmacists). Regarding the current capacity of the nursing staff: 84% of the nursing staff self-assessed their ability to complete at a good level or higher the tasks according to regulations in the following contents: organizing health care; directing the hygiene work of departments and rooms; managing human resources.