+ Protective function: EI Sinhennhicop and Gross believed that the appendix has many lymphatic clusters that play an important role in the body's defense against germs. The appendix's infection-prevention function (the lymphatic system in the appendix) is no less important than the function of the lymphatic system of the tonsils in the pharynx.
+ Digestive function: the appendix secretes alkaline fluid, including enzymes such as Amylase, Pepsin and mucus. In 24 hours, the adult appendix secretes about 2ml of mucus, Amylase and Protide-digesting enzymes.
1.3 APPENDICULAR ABSCESS
1.3.1 Clinical symptoms
- Extraperitoneal abscess
Maybe you are interested!
-

 Study on imaging characteristics and value of multi-slice computed tomography in diagnosing acute appendicitis - 2
Study on imaging characteristics and value of multi-slice computed tomography in diagnosing acute appendicitis - 2 -
 Internal control of revenue and expenditure activities at the National Children's Hospital - 2
Internal control of revenue and expenditure activities at the National Children's Hospital - 2 -
 Statistics By Job Position At Viet Duc Friendship Hospital
Statistics By Job Position At Viet Duc Friendship Hospital -
 Development Strategy of Duc Giang General Hospital to 2025
Development Strategy of Duc Giang General Hospital to 2025 -
 Study on microbiological characteristics of foot ulcers in diabetic patients at the Department of Endocrinology - Diabetes, Bach Mai Hospital in 2021 - 11
Study on microbiological characteristics of foot ulcers in diabetic patients at the Department of Endocrinology - Diabetes, Bach Mai Hospital in 2021 - 11
When the appendix is close to the lateral, posterior or posterior abdominal wall such as the appendix after the cecum when it ruptures, the adjacent organs and the greater omentum will enclose the abscess, isolating it from the remaining organs in the abdominal cavity by the inner wall, and the outer wall is the abdominal wall. Examination shows a mass attached to the anterior or posterior abdominal wall, continuous with the iliac crest, a round, tense mass, clear boundaries, painful to press, sometimes about to burst through the skin, making us see clearly the signs: swelling, heat, redness, pain. In this case, it is necessary to further differentiate from abdominal wall abscess and pelvic muscle abscess, differentiate from cecal tumor invading the abdominal wall. Ultrasound and colonography are needed for definitive diagnosis. Treatment: puncture at the most painful, most swollen, most tense point, closest to the abdominal wall, preferably puncture under ultrasound guidance and follow the puncture needle to incise and drain the extraperitoneal pus, it is not necessary to remove the appendix. If the appendix is not seen when incised, just drain the pus to completely expose the skin and schedule the patient to have surgery to remove the appendix in 6 months.
- Intraperitoneal appendiceal abscess
When the appendix is located around the mesentery, the ruptured appendix is localized by the mesenteric roots, intestinal tracts, and greater omentum. The patient often has a high fever with symptoms of intestinal obstruction or partial intestinal obstruction. Examination shows a tumor near the right navel, far from the abdominal wall, with clear boundaries, very painful to press, not mobile. X-rays show signs of intestinal obstruction, ultrasound shows the image of an abscess. In this case, it is necessary to operate on the abdomen, drain the abscess, remove intestinal adhesions, restore the circulation of the digestive tract, and clean the abdomen.
- Pelvic abscess
When the ruptured appendix is located behind the pelvis, the patient often has pain in the lower abdomen, the right iliac fossa has little pain and vague pain, the abdominal wall reaction is unclear, mainly pain in the right suprapubic bone, high fever fluctuates. There is frequent urination, painful urination, even urinary retention. There are symptoms of digestive disorders similar to dysentery: colic pain, urge to push out mucus and blood in the stool, rectal and vaginal examination of the Douglas pouch and the right fornix shows pain, the anal sphincter is loose, ultrasound shows an abscess in the pelvis. If drained, the pus is passed through the Douglas pouch, only after 6 months the patient is scheduled for surgery again to remove the appendix.
1.3.2. Diagnostic imaging of appendicitis
1.3.2.1. Ultrasound

Figure 1.3 Ultrasound image of appendiceal abscess
* Source: Medlatec Hospital [17]
Due to the nature of the fluid, the phenomenon of sound enhancement behind the abscess is very clear, the pus often has no echo or has echogenic particles inside the fluid, sometimes there is the presence of air bubbles condensing above the abscess or scattered in the pus of the abscess. Doppler ultrasound examination shows congestion on the wall of the abscess showing an increase in Doppler signal.
1.3.2.2. Computed tomography
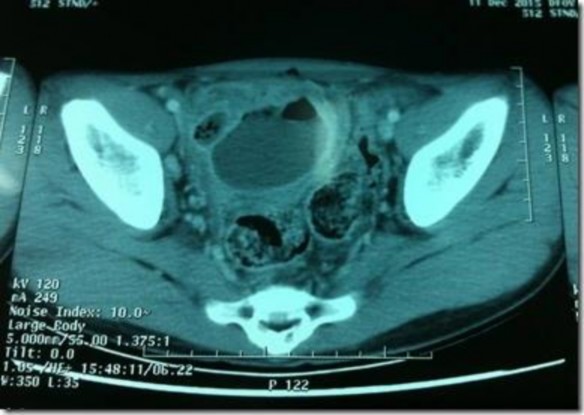
Figure 1.4 Image of appendiceal abscess on CT scan
*Source Dr Mohamed Saber [18]
Fluid collection is seen in the appendicular region with or without air within. Many times an appendicolith may be visualized [18].
There is an image of an abscess in the right iliac fossa, an image of a ruptured appendix, sometimes fecal stones are seen inside the abscess.
It is best to take a contrast image to accurately diagnose appendiceal abscess and differentiate it from other causes.
1.3.3. Other paraclinical
1.3.3.1. Blood formula
Leukocytes: In most AXRTs there is usually a clear increase > 10,000 BC/mm³
1.3.3.2. Microbiology of appendiceal abscess
+ Aspirate to determine the pus of the abscess: pus is usually opaque white, sometimes yellow-green, with a very foul smell.
+ Daniel T. Cloud believes that bacteria (VK) causing VRT and AXRT are bacteria that normally live in the colon, the most important is Bacteroides fragilis , an anaerobic bacteria (VKKK), followed by Escherichia coli ( E. coli ), a partially aerobic bacteria (VKHK) [15]
+ Through research by many authors, it has been shown that: although the results of isolation of bacterial strains are different in terms of ratio, identification or naming over time, there is a common conclusion that there is a mixed infection by bacterial strains, in which E. coli is prominent , along with bacterial strains represented by B. Fragilis [16] .
1.3.4. Complications of appendiceal abscess
The AX can rupture posteriorly into the iliopsoas muscle mass and cause AX of this muscle, causing many difficulties in treatment, or rupture into the abdominal cavity, causing VPM, or rupture outside the skin, more rarely into the retroperitoneal space, sometimes rupture into adjacent hollow organs such as the colon, small intestine, bladder, or rarely rupture into the fallopian tube.
1.4. TREATMENT METHODS
1.4.1 Treatment principles
- Mainly medical treatment, appendectomy when the patient has pain again after discharge from the hospital or at least 2 months after discharge from the hospital
- Emergency surgery when the abscess is at risk of rupture causing peritonitis, failure after medical and surgical treatment
- Place a nasogastric tube if the patient has severe abdominal distension, vomiting or suspected associated injury.
- Perform pathological examination and antibiotic susceptibility testing during surgery.
* For abscesses whose wall has adhered to the abdominal wall, drain the abscess extraperitoneally. For abscesses in the HCP, the incision is parallel to the femoral arch, 1 cm above the anterior iliac spine. The drainage incision is above the anterior iliac crest, 2 cm above the posterior cecal abscess. Drainage is through the anterior rectal wall if the abscess is in the Douglas pouch. The appendix will be surgically removed after 3-6 months.
* For abscesses located in the middle of the mesentery, not attached to the abdominal wall, open the abdominal cavity to drain the abscess and remove the appendix in one step.
1.4.2 Internal medicine
- Use broad-spectrum antibiotics (2nd and 3rd generation Cephalosporins) combined with Metronidazole. For appendiceal abscesses with a pus size < 4cm, only medical treatment is needed. For appendiceal abscesses with a size ≥ 4cm, use antibiotics and drain pus under ultrasound guidance.
- Monitor blood count, erythrocyte sedimentation rate, clinical response and ultrasound after 3 days and 7 days of treatment. If the abscess is still large, perform a second, third, etc. pus aspiration.... [19]
- Indication for ultrasound-guided pus drainage
Ultrasound-guided drainage of pus with RT abscess in HCP, size > 4cm and no complications of rupture into organs or peritoneal cavity.
a, Pus aspiration process
- Prepare patient and instruments
- Position of the operator: Stand on the right side of the patient if the needle is inserted from the outside in towards the navel, upwards or downwards. Stand on the left side if the needle is inserted perpendicularly or obliquely to the abdominal wall plane.
* Pus aspiration technique
- Select puncture site: The puncture site must comply with the following principles: Access to the pressure socket
- shortest path. The needle avoids going through blood vessels and intestines. Use doppler technique and pressure on the probe to find the safest way into the abscess.
- Anesthesia of puncture area:
+ Use 3-5ml of xylocaine or lidocaine 1% to anesthetize each layer of the abdominal wall in the direction of the needle puncture. Anesthesia for children.
+ Disinfect the puncture area: Use Betadine solution or jode to widely disinfect the puncture area in a centrifugal direction.
- How to poke & Enjoy poking:
+ Method 1: With probe without holder, no software
Instructions: needle puncture direction is consistent with the tip of the probe at an angle > 0° - 45° depending on the location and guidance of the abscess cavity entrance of the SÂ.
+ Puncture method 2: With the probe type that comes with a needle holder and software
Aspiration instructions, the needle puncture direction is almost always at a 45° angle to the axis of the red tip. With this method, it can be applied to puncture any location and size of abscess. Insert the needle from the abdominal wall, when the needle tip reaches the peritoneum, tell the patient to. Temporarily stop breathing, quickly insert the needle tip into the abscess cavity and then aim towards the center of the abscess, when the needle is completely inside the abscess, tell the patient to exhale gently and regularly.
- Pus aspiration: do not fix the needle but let the needle move with the breathing rhythm and aspirate pus under ultrasound monitoring, while aspirating, adjust the needle close to the bottom and directions of the pus pocket, avoid letting the needle tip puncture the inner wall of the pus pocket causing bleeding.
- Rinsing the abscess: When thick pus mixed with necrotic tissue blocks the needle or makes it difficult to drain the pus, inject 5 - 10ml of saline solution, drain it and continue rinsing. Inject 160ng of Gentamycine and drain it all again at the end of the procedure.
- Assess the completeness of pus based on: The amount of pus aspirated compared to the estimated volume. The pus is initially thin, then becomes thicker. The ultrasound will show that the hypoechoic area gradually shrinks and the hyperechoic area becomes clearer. If all the pus is aspirated, the hypoechoic area will no longer be visible. Quickly withdraw the needle in the direction it was inserted.
- Pus testing and antibiotic susceptibility testing: Pus is collected using a plastic syringe with a volume of 3-5 ml and a plastic cap is used to cover the tip of the needle.
, transfer the pus sample immediately after suction within 15 minutes. [16] b, Antibiotic treatment
Before and after aspiration, the patient was treated with a combination of 2 of 3 types of empirical antibiotics and topical antibiotics, the dosage depending on body weight and drug tolerance: Gentamicin or a third-generation Cephalosporin combined with Metronidazole.
c, Early results assessment
- Good: When only aspirated once, clinical improvement is rapid, BC and VS tests return to normal or decrease rapidly, the abscess image on ultrasound is gone, there are no complications, hospital stay is less than 10 days.
- Average: When pus must be aspirated a second or third time, there is no evidence of infection and severe complications, treatment time is over 10 days.
- Bad: When having to puncture more than 3 times, the puncture technique causes complications such as puncture into the intestines, bladder... causing complications of red digestive fluid, urine or puncture into blood vessels causing severe bleeding in the abdomen.
d, Long-term assessment of results