LIST OF TABLES
Table 1.1: Alvarado 9-point scale
Table 2.1: Comparison of CLVT results with GPB results 23
Table 3.1: Location of appendix on CT scan 25
Table 3.2: Appendiceal diameter size on CT scan 27
Maybe you are interested!
-

 Study on microbiological characteristics of foot ulcers in diabetic patients at the Department of Endocrinology - Diabetes, Bach Mai Hospital in 2021 - 11
Study on microbiological characteristics of foot ulcers in diabetic patients at the Department of Endocrinology - Diabetes, Bach Mai Hospital in 2021 - 11 -
 Study on botanical characteristics, chemical composition and acetylcholinesterase enzyme inhibitory effects of two species Piper thomsonii (C. DC.) Hook. f. var. thomsonii and Piper hymenophyllum Miq., Piperaceae family - 24
Study on botanical characteristics, chemical composition and acetylcholinesterase enzyme inhibitory effects of two species Piper thomsonii (C. DC.) Hook. f. var. thomsonii and Piper hymenophyllum Miq., Piperaceae family - 24 -
 Study on natural regeneration characteristics of Lim xet tree species Peltophorum tonkinensis A.Chev in Lam Binh district, Tuyen Quang province - 13
Study on natural regeneration characteristics of Lim xet tree species Peltophorum tonkinensis A.Chev in Lam Binh district, Tuyen Quang province - 13 -
 Study on botanical characteristics, chemical composition and acetylcholinesterase enzyme inhibitory effects of two species Piper thomsonii (C. DC.) Hook. f. var. thomsonii and Piper hymenophyllum Miq., Piperaceae family - 23
Study on botanical characteristics, chemical composition and acetylcholinesterase enzyme inhibitory effects of two species Piper thomsonii (C. DC.) Hook. f. var. thomsonii and Piper hymenophyllum Miq., Piperaceae family - 23 -
 Study on botanical characteristics, chemical composition and acetylcholinesterase enzyme inhibitory effects of two species Piper thomsonii (C. DC.) Hook. f. var. thomsonii and Piper hymenophyllum Miq., Piperaceae family - 21
Study on botanical characteristics, chemical composition and acetylcholinesterase enzyme inhibitory effects of two species Piper thomsonii (C. DC.) Hook. f. var. thomsonii and Piper hymenophyllum Miq., Piperaceae family - 21
Table 3.3: Evaluation of RT wall thickness on CLVT 28
Table 3.4: Assessment of signs of fatty infiltration on CT 28
Table 3.5: Other signs on CLVT 30
Table 3.6: Diagnosis of appendiceal rupture complications on CT 30
Table 3.7: Comparison of CLVT with Alvarado scale 31
Table 3.8: Value of Alvarado score in diagnosing VRTC 32
Table 3.9: Comparison of CT scan with ultrasound 32
Table 3.10: Value of ultrasound in diagnosing VRTC 33
Table 3.11: Conclusion of CLVT 33
Table 3.12: Assessment of the location of the appendix 34
Table 3.13: Value of CT in diagnosing appendix diameter 34
Table 3.14: Value of CT in diagnosing RT rupture complications 35
Table 3.15: Value of CLVT in diagnosing VRTC 35
Table 4.1: Comparison of the value of CLVT in diagnosing VRTC of 45 studies
LIST OF IMAGES
Figure 1.1: Anatomical location of the appendix 3
Figure 1.2: Gross image of appendicitis 4
Figure 1.3: Examination of VRTC signs 7
Figure 1.4: Typical appendicitis 10
Figure 1.5: Non-contrast CT scan of VRTC patient 15
Figure 1.6: CT scan with contrast injection on patient with VRTC 16
Figure 1.7: Image of VRTC with calcification, forming an abscess 16
Figure 3.1: Distribution of VRTC patients by age 24
Figure 3.2: Distribution of VRTC patients by gender 25
Figure 3.3: The appendix is located behind the cecum, with fecal stones inside. 26
Figure 3.4: The appendix is located in the pelvic area, with fecal stones inside.
Figure 3.5: Appendix increased in size 27
Figure 3.6: Image of fat infiltration around RT 29
Figure 3.7: Complications of ruptured appendix on CT scan 31
Figure 3.8: Patient Nguyen Thi X. was diagnosed with VRTC on CT scan 36
PROBLEM STATEMENT
Acute appendicitis (AP) is one of the most common causes of abdominal emergencies and one of the most common indications for emergency abdominal surgery worldwide [41]. Acute appendicitis can occur at any age but is most common between the ages of 10 and 20. The lifetime risk of acute appendicitis is 8.6% in men and 6.9% in women; the rate of appendectomy is 12% in men and 23% in women [24]. The rate of perforation of the appendix ranges from 16 to 40%, with higher frequencies in younger people (40-57%) and in patients over 50 years of age (55-70%). Perforation of the appendix is associated with increased mortality compared with acute appendicitis without perforation. The risk of death in patients with non-necrotizing appendicitis is less than 0.1% but the risk increases to 0.6% in necrotizing appendicitis. On the other hand, perforation of the appendix has a higher mortality rate of approximately 5%. The clinical diagnosis of acute appendicitis can be straightforward in patients with typical signs and symptoms, but atypical presentations can lead to diagnostic confusion and delays in treatment. Diagnosis usually involves a combination of clinical, laboratory, and imaging findings. Accurate diagnosis of appendicitis remains a challenge because clinical signs or positive blood test results may be absent in up to 55% of patients. Diagnostic yield may be improved by using clinical scales that correlate with examination and assessment of inflammatory markers. The role of imaging studies such as ultrasound, computed tomography, or magnetic resonance imaging is controversial [19, 43, 44].
There are three commonly used imaging modalities for diagnosis: Ultrasound, computed tomography, and magnetic resonance imaging. Abdominal ultrasound is the first-line method, but abdominal computed tomography is superior to ultrasound. CT is an adjunct to ultrasound and is recommended when ultrasound results are suboptimal, indeterminate, or normal in patients with acute abdominal pain [19, 35].
Each year, according to reported rates, approximately 20-40% of cases of appendicitis are missed during diagnosis. The negative appendectomy rate is
reported to range from 10%-34% [43]. Therefore, accurate diagnosis of appendicitis is an issue that needs more attention.
In order to diagnose early and accurately the symptoms on CT scans and evaluate the effectiveness of using multi-slice computed tomography in diagnosing acute appendicitis, we conducted the project : "Research on imaging characteristics and value of multi-slice computed tomography in diagnosing acute appendicitis." with 2 objectives:
1. Describe the imaging characteristics of acute appendicitis on multi-slice CT scan.
2. Evaluation of the value of multi-slice CT scan in the diagnosis of acute appendicitis.
Chapter 1
DOCUMENT OVERVIEW
1.1. OVERVIEW OF EPIDEMIOLOGY OF ACUTE APPENDICITIS
Acute appendicitis (AP) is a common cause of acute abdominal pain, with an incidence of approximately 1/1000 people per year, and a lifetime risk of 7–9% in developed countries [22].
According to a study by Ferris et al. in 2017, the number of appendicitis and appendectomy cases was up to 100/100,000 cases per year [26].
Delayed or incorrect diagnosis of VRTC can lead to serious complications such as perforation, abscess formation, peritonitis, and sepsis. Therefore, accurate and timely diagnosis is required to avoid complications of delayed surgery or unnecessary surgical intervention [43].
1.2. GPB, PATHOGENESIS OF ACUTE APPENDICITIS
1.2.1. Appendiceal anatomy
The appendix is a small, narrow tube attached to the cecum. Grossly, the appendix is 1-25 cm long, however, its size usually varies between 5-10 cm [21].
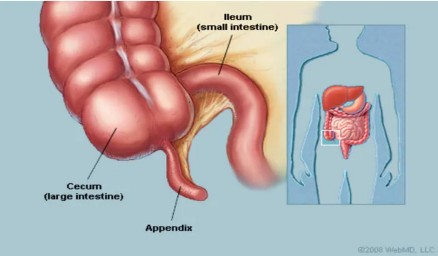
Figure 1.1: Anatomical location of the appendix
In terms of microscopic structure, the appendix wall consists of 4 layers, from inside to outside: mucosa, submucosa, muscular layer and serosa [21]. Outside the serosa is a thin layer of peritoneum covering. The muscular layer includes circular muscle on the inside.
inner and longitudinal muscle on the outside. The submucosa contains connective tissue and lymphoid tissue [28].
1.2.2. Pathological anatomy of appendicitis
Grossly, the appendix was inflamed, swollen, edematous, congested blood vessels were prominent under the serosa, fibrinous exudate formed a pseudomembrane on the serosa surface, and pus was seen flowing from the appendix when the appendix was split in half [2].

Figure 1.2: Gross image of appendicitis
Microscopic images of appendicitis have three main characteristics: congestion, inflammatory edema, and cellular infiltration (mainly neutrophils) [2].
Based on the pathological results, it is possible to determine whether the appendix is actually inflamed or not. Therefore, the pathological results help to confirm the diagnosis of acute appendicitis.
1.2.3. Pathogenesis
The cause and mechanism of acute appendicitis are due to obstruction in the lumen of the appendix and infection. In children and young adults, the cause of obstruction of the lumen of the appendix may be due to proliferation of lymphoid follicles. At birth, these lymphoid follicles are small in number, then gradually increase in number in adulthood and increase in size when infected with bacteria or viruses. In adults, the cause of obstruction of the lumen of the appendix is often due to fecal stones. In addition, it may also be due to foreign bodies, roundworms, pinworms, benign or malignant tumors [3, 41].
Obstruction leads to inflammation, ischemia, and bacterial overgrowth. If left untreated, necrosis and perforation of the appendix occur. When the appendix is obstructed, there is increased pressure within the appendix, leading to occlusion of small vessels and lymphatic congestion. Once obstruction occurs, the appendix fills with mucus and becomes distended. As lymphatic and vascular damage progresses, the appendix wall becomes ischemic and necrotic. This is followed by overgrowth of aerobic bacteria in the early stages and mixed aerobic or anaerobic bacteria in the late stages. Once significant inflammation and necrosis occur, the appendix is at risk of perforation. If the perforation is blocked by the omentum, an abscess forms [17, 38]. In cases where pus flows freely into the peritoneal cavity, it causes generalized peritonitis [11].
In some cases of appendicitis that has not ruptured, the surrounding tissues also react, creating a protective layer, forming an appendiceal mass [11].
1.3. CLINICAL SYMPTOMS AND TESTS TO DIAGNOSIS OF ACUTE APPENDICITIS
The diagnosis of appendicitis currently still depends mainly on typical clinical symptoms. Clinicians need to master clinical symptoms and tests to be able to make an accurate diagnosis, then perform appropriate imaging diagnostic methods to ensure the best interests of the patient.
1.3.1. Clinical features
1.3.1.1. Systemic symptoms
The early signs of appendicitis are often subtle. Routine physical examination may not detect them in the early stages of the disease [41].
Common systemic symptoms are fever of 37.5-38℃ [11]. Most sick children have body temperatures above 37℃ [27]. The elderly may not have fever. About 20% of patients are pregnant women with fever above 37.8℃ [18]. VRTC often has a low fever. When the temperature is above 38.3℃, perforation should be suspected [19].
Symptoms of infection: gaunt face, dry lips, dirty tongue, bad breath, general fatigue, etc.
1.3.1.2. Functional symptoms
Abdominal pain is a common symptom, especially in the right iliac fossa [4]. The classic symptom first described by patients is abdominal pain. Initially, the pain may be in the supraumbilical or periumbilical region and then gradually localized to the right iliac fossa [11]. However, patients may also describe severe, intermittent pain in the first 24 hours, then continuous pain that moves to the right iliac fossa [19]. Sometimes the location of pain is atypical due to anatomical changes in women in the third trimester of pregnancy due to increased uterine size [18].
Nausea and vomiting are common symptoms, especially in children [11]. These symptoms often occur after the onset of pain [47]. When the patient describes vomiting occurring before abdominal pain, the diagnosis should be reassessed.
In addition, there are some symptoms of digestive disorders such as: loss of appetite, bloating, indigestion, constipation, diarrhea [11, 41]. These symptoms are not specific.
The initial symptoms of VRT are often very discreet and easily overlooked. Therefore, to diagnose VRTC early and accurately, doctors need to ask questions carefully, combine symptoms and prescribe appropriate paraclinical tests.
1.3.1.3. Physical symptoms
Physical symptoms are symptoms that doctors identify through clinical examination. It is necessary to gently examine from the painless area to the painful area to detect abnormal signs of the abdominal wall:
When performing a clinical examination, attention should be paid to the following pain points:
McBurney point: located midway between the anterior superior iliac spine and the umbilicus. The patient feels pain when the doctor performs the pressing movement.
Lanz point: line connecting the right 1/3 and left 2/3 of the anterior iliac spine line
above.
Clado point: is the intersection of the anterior superior iliac spine line and the border
outside the right rectus abdominis muscle.