themselves, helping children to be more interested in doing the Valsalva maneuver every day. The authors also use the Politzer or modified Politzer maneuver
Advantages: The above methods can be performed at home or with the assistance of a physician without the need for invasive surgery. Williamson120In a study of 2 groups of 160 children treated with Otovent compared with other methods, the rate of improvement in B-form tympanogram was 49.6% compared with 38.3%. De Nobili121showed that performing Otovent balloon inflation for less than 1 month improved hearing by 10dB. Rosso122Otovent balloon therapy improves short- and medium-term hearing thresholds and VTGUD in children with KHVM, leading to earlier improvement in auditory performance.
Disadvantages: Only applicable to children who are old enough, usually over 4 years old, without acute rhinopharyngitis.
1.6.2 Tympanic membrane ventilation tube placement surgery
Maybe you are interested!
-
 Indications and Some Technical Characteristics of Laparoscopic Surgical Methods
Indications and Some Technical Characteristics of Laparoscopic Surgical Methods -
 Study on the nutritional effectiveness of homemade high-energy solution for early feeding through nasogastric tube for critically ill patients at Hue Central Hospital - 1
Study on the nutritional effectiveness of homemade high-energy solution for early feeding through nasogastric tube for critically ill patients at Hue Central Hospital - 1 -
 Legal Status on the Content of Industrial Property Rights for Geographical Indications
Legal Status on the Content of Industrial Property Rights for Geographical Indications -
 Protection of industrial property rights for geographical indications under Vietnamese law - Ninh Thi Thanh Thuy - 2
Protection of industrial property rights for geographical indications under Vietnamese law - Ninh Thi Thanh Thuy - 2 -
 State the Purpose - Indications - Contraindications of Enemas - Retention Enemas. 2-List the Types of Solutions Used for Enemas - Retention Enemas.
State the Purpose - Indications - Contraindications of Enemas - Retention Enemas. 2-List the Types of Solutions Used for Enemas - Retention Enemas.
1.6.2.1 General
A tympanic membrane ventilation tube is a small tube placed over the eardrum to maintain a hole in the eardrum with the goal of ensuring temporary tympanic membrane ventilation, draining tympanic fluid, and rapidly improving symptoms, most importantly hearing.
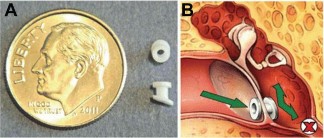
Figure 1.8 Tympanic membrane ventilation tube
A. The size of the OTK is about the size of a coin. B. The OTK allows air to flow directly into the middle ear, helping with ventilation in cases of reduced Eustachian tube function.
(Source: Rosenfeld 123 , 2005)
There are many types of ventilation tubes with different sizes and materials such as: titanium, fluorplastic, silicone... Tube diameter can range from 0.76mm - 1.56mm used depending on age and viscosity of fluid.124Based on the time OTK stays on the eardrum, OTK is divided into 3 main types: short-term type (from 6 to 12 months); intermediate type (from 9 to 14 months), long-term type: usually T-shaped (about 2-3 years).47
1.6.2.2 Indications for tympanic membrane ventilation tube placement in children with KHVM
Paradise22(1969) in a study on KHVM patients noted that VTGUD was very common in children with KHVM, so he proposed placing OTK through the tympanic membrane in all children born with cleft.
According to the 2013 clinical practice guidelines of the American Academy of Otolaryngology - Head and Neck Surgery, children with craniofacial abnormalities such as KHVM have a higher rate of VTGUD, hearing loss, and delayed language development than normal children, so early intervention is needed for this group. 125,126 Thus, in the world, OTK placement in children with KHVM is indicated earlier and more widely than in children with VTG not due to malformation, including VTGUD and recurrent VTGCT.
In Vietnam, according to the technical process of examination and treatment of ENT diseases issued by the Ministry of Health in 2012, OTK placement is indicated in the following cases: Serous otitis media; Eustachian tube obstruction due to adenoids; Eustachian tube obstruction due to nasopharyngeal tumors (such as nasopharyngeal cancer); Otitis media with a hole too small to drain pus.127However, there are no specific instructions in the above cases, nor are there any recommendations on placing OTK in special, high-risk subjects such as children with KHVM.
1.6.2.3 Results and complications
Result
According to authors around the world, placing an OTK tympanic membrane can immediately correct hearing loss and fluid in VTGUD, as well as prevent chronic progression of the disease.
According to Rosenfeld103(2004), the rate of tympanic membrane returning to normal after OTK placement was 62%, PTA increased from 6 - 12 dB after OTK placement. According to Nguyen Dinh Truong19 , after 3 months of OTK placement, 60% of middle ears returned to normal, 34.3% had fluid retention after the ventilation tube fell out and needed to be re-placed. Audiogram improved with an average PTA of 17.25 dB.
Complications
OTK placement may have unwanted complications. After OTK placement, it is necessary to monitor the tube blockage, tube discharge, and tube retention time on the tympanic membrane. Otorrhea is the most common complication after OTK placement surgery through the tympanic membrane with a rate ranging from 3.4% to 96.9%.51,128 According to Ginny Curtin 129 the frequency of otorrhea is 0.79 episodes in 6 months and 1.5 episodes in 12 months. According to Erdoglija and Sotirovic (2012) 130 the tube blockage rate is 9.5%. Early OTK blockage or fallout when Eustachian tube function has not recovered leads to recurrent VTGUD or VTGCT. According to Nguyen Dinh Truong 19 , the condition of OTK being pushed out before 6 months after surgery is an early complication with a rate of 20/35 ears.
According to Kay and Nelson (2001)124The sequelae of OTK placement are atrial fibrosis at a rate of 32%; atrial collapse at 25%; retraction pouch at 3.1% and cholesteatoma at 0.7%. According to Mengkhim131 , tympanic membrane perforation after OTK placement 3 months occurred in 4/65 ears (6.1%). In addition, there may be some rare late complications such as OTK slipping into the tympanic cavity and sensorineural deafness.
1.6.3 The role of palate surgery
The role of palatopharyngoplasty in the rehabilitation of the Eustachian tube-middle ear has been studied by many authors. Some studies have found that palatopharyngoplasty is associated with a reduced risk of Eustachian tube pathology in children (5 years and older), but the results have not been conclusive.93,132 Hassan 133 found that three-layer palatopharyngoplasty was more effective than two-layer surgery in reducing recurrent otitis media with effusion. Carroll 134 operated on 69 3-year-old patients, and after 3 years, the rate of conductive hearing loss of more than 20 dB decreased from 30.4% to 13.0%. Using a Z-flap gave better results with PTA at 10.0 dB after surgery.
However, in the short term, there is little or no evidence that THVMs resolve eustachian tube dysfunction or otitis media with effusion135,136 . Sunil137A study of two groups of children who underwent cleft palate surgery at age 6 and before age 2 found that 56.6% in group A and 40.6% in group B had normal otoscopy results, and 20% of the group had type A tympanograms. According to Nguyen Van Ninh et al.32(2016), in KHVM patients without palateplasty, the rate of VTGUD was 71.5% out of a total of 91% of middle ear diseases. The rate of VTGUD and middle ear diseases decreased in the surgical group but was still high at 47.6% and 73.8%, respectively. 32. According to Khieu Huu Thanh and Luong Thi Minh Huong 3 , in KHVM patients with VTGUD, the rate of VTGUD ears before and after 6 months of palateplasty was 91.9% and 85.7%, respectively.
Thus, it is necessary to combine OTK surgery to treat middle ear pathology in children with KHVM while waiting for the results of improving the function of the Eustachian tube of THVM surgery and the child's development.
CHAPTER 2
RESEARCH OBJECTS AND METHODS
2.1 SUBJECTS OF RESEARCH
2.1.1 Research subjects
Secondary cleft palate patients with middle ear disease were treated with palateplasty combined with tympanic membrane ventilation.
The selected subjects are children under 16 years old, regardless of gender, ethnicity, or place of residence.
2.1.1.1 Selection criteria
Objective 1:
Patients with secondary cleft palate, possibly with cleft lip
There is an indication for palate shaping.
Endoscopic examination, tympanometry, possibly with audiometry
Objective 2:
Middle ear disease diagnosed by otoscopy: otitis media with effusion, recurrent acute otitis media, grade II-III tympanic collapse.
Had palate surgery.
Had tympanic membrane ventilation surgery.
Be followed up for at least 12 months.
Subject or guardian agrees to participate in the study
2.1.1.2 Exclusion criteria
Objective 1:
Patients with KHVM in syndromes have other congenital malformations causing facial deformities.
Objective 2:
Patients who drop out of treatment or are not adequately followed up
2.1.2 Research location
Vietnam - Cuba Friendship Hospital, Hanoi.
2.1.3 Research time
From January 2016 to December 2019.
2.1.4 Steps of selection into research
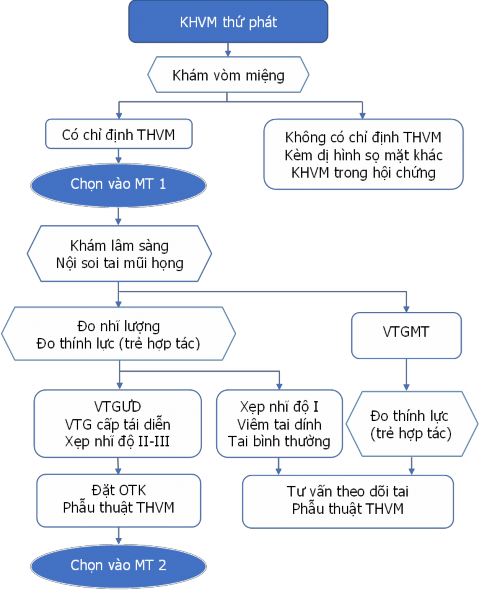
Figure 2.1 Diagram of selecting research subjects
2.2 RESEARCH METHODS
2.2.1 Research design
Prospective, descriptive study of case series with clinical intervention, no control group.
2.2.2 Number of study patients
In the study, we used purposive sampling method . Objective 1:
106 children with secondary cleft palate were indicated for palateplasty, endoscopic examination, tympanometry, possibly accompanied by audiometry.
Objective 2:
183 ears were diagnosed with recurrent atrial septal defect, atrial septal defect, and grade II-III atrial collapse in 106 children with congenital atrial septal defect who underwent palate reconstruction surgery combined with tympanic membrane perforation (77 children had bilateral membrane perforation, 29 children had unilateral membrane perforation).
2.2.3 Steps to conduct research
Step 1: Through the outline, build a sample medical record.
Step 2: Clinical examination, paraclinical examination and surgical indication
Patients indicated for THVM surgery at Vietnam Cuba Hospital are examined for functional symptoms, and have their ears, nose, throat, and palate examined.
Assess middle ear condition by endoscopy, measure tympanic membrane if tympanic membrane is intact, measure pure tone audiometry if child is cooperative.
Diagnosis of middle ear disease: definitive diagnosis by endoscopy, can be combined with functional symptoms, tympanometry or audiometry.
Step 3: Palatal plastic surgery and tympanic membrane implant placement
Patients are indicated for OTK placement when diagnosed with otitis media with effusion, recurrent acute otitis media, and grade II-III tympanic collapse.
OTK placement surgery is performed by an ENT doctor, immediately after THVM surgery, under the same anesthesia. Intraoperative assessment of the condition of the middle ear and fluid in the tympanic cavity.
THVM surgery is performed by a trained Maxillofacial Surgeon or Plastic Surgeon who has agreed on the surgical procedure.
Step 4: Patients after KHVM surgery combined with OTK placement are monitored for at least 12 months.
Palatal examination, evaluation of THVM results at 6 months.
Otoscopy to assess the condition of the ventilation tube, eardrum, and middle ear disease at 3 months, 6 months, and 12 months.
Evaluation of middle ear function after 6 months and 12 months depending on the condition of the tympanic membrane by endoscopy:
Tympanic membrane with OTK or OTK falls but tympanic membrane perforation remains: pure-tone audiometry (on cooperative children).
OTK falls, tympanic membrane intact: tympanometry, pure tone audiometry (on cooperative children).
Step 5: Process data and write thesis.
2.2.4 Research variable indicators
2.2.4.1 Objective 1
* General characteristics
- Age: children under 5 years old are calculated by month. Children over 5 years old are calculated by age. Divided into age groups: 12 - 24 months; >24 - 36 months; >36 - 48 months; >48 - 60 months and over 5 years old.
- Gender: male and female