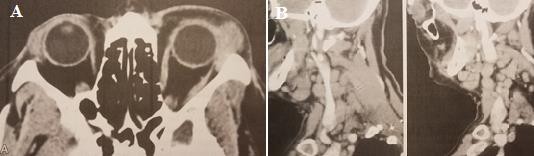
Figure 1.11. Computed tomography of malignant lymphoma of lacrimal gland
A. Left eye has a tumor in the lacrimal fossa . B. Lymph nodes in the neck Source: Coupland et al. (1998)48
+ Histopathology
Extranodal marginal zone lymphoma (EMZL) is characterized by a dense infiltration of small cells with extensive cytoplasm, slightly wrinkled nuclei, and absent nucleoli resembling marginal zone cells. Plasmacytic differentiation is common with prominent Dutcher bodies. Scattered centroblast-like and immunoblastic cells are present, along with marginal zone cells. Immunohistochemically, EMZL is positive for B-cell lineage markers such as CD79a and CD20. Furthermore, most cases of EMZL are positive for BCl2 and negative for CD5, CD10, CD23, and
Cyclin D1.49
Follicular lymphoma (FL) is a lymphoma of the follicular B cells.49Immunohistochemically, FL is positive for CD79a, CD20 and centroblast markers CD10, BCl6 in most cases. About 90% of FL overexpresses BCl2. FL is negative for CD5. Furthermore, FL is classified based on the number of centroblasts per high-power field (HPF): grade 1 (0-5/HPF), grade 2 (6-15/HPF) and grade 3 (>15/HPF). Grade 3 is divided into grade 3A if centroblasts are present.
grade 3B if only centroblastoma is present. Grade 3B resembles DLBCL clinically and biologically.
Diffuse large B-cell lymphoma (DLBCL) is a biologically, clinically, and histopathologically diverse disease. The general definition of DLBCL is a tumor consisting of a diffuse proliferation of large B cells with nuclear size twice that of normal lymphocytes or equal to/larger than that of normal macrophages (centroblast morphology).49Other common morphological variants include: Immunoblastic type with nuclear-nucleated cells
centrally located, with extensive basophilic cytoplasm and anaplastic type with large polygonal or oval cells, pleomorphic nuclei. Immunohistochemically, tumor cells are positive for CD79a and CD20. About 10% of tumor cells are positive for CD5, 50% are positive for CD10. Expression of CD30 is characteristic of anaplastic DLBCL. High proliferative activity (> 40%) is revealed by Ki67.49
Follicular cell lymphoma arises from B cells of the follicular zone within the germinal center. Morphologically, the tumor consists of a monomorphic pattern of small to medium-sized lymphocytes with narrow cytoplasm, irregular nuclei, indistinct nucleoli, and absence of transformed large cells. The tumor cells overexpress Cyclin D1, are positive for CD20, CD79a, BCl2, and are negative for CD3, CD10, CD23, and BCl6.
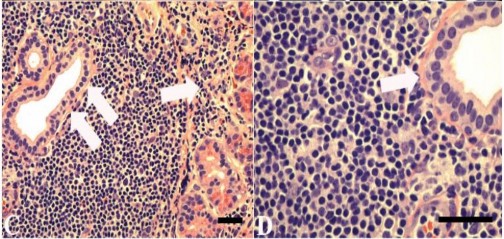
Figure 1.12. Histopathological features of malignant marginal zone lymphoma
Source: Knowles et al. (1990)50
Knowles et al. (1990) studied 108 patients with lymphoma and showed that it was not necessary to distinguish between lymphoproliferations of lacrimal origin and other origins, and that the pathophysiological features did not differ between the two groups. However, due to advances in immunology and genetics, the authors re-studied malignant ocular lymphomas and applied new techniques. In the primary malignant lymphoma group, malignant extranodal marginal zone lymphoma (EMZL) accounted for a high proportion. In the secondary malignant lymphoma group, follicular lymphoma (FL) accounted for a high proportion. Usually, pathological samples from the lacrimal gland or from ocular lesions contained infiltrating lymphocytes, making it difficult to distinguish between lymphoproliferations.
benign or malignant. In these cases, immunology and genetic analysis are needed for definitive diagnosis.50
According to Liesegang et al. (1993), proliferative lesions are a very broad category, including reactive lymphoid hyperplasia, atypical lymphoid hyperplasia, and malignant lymphoma.51These hyperplasias are difficult to distinguish. The two types of hyperplasia can progress to either localized or systemic malignant lymphoma. Similar lesions can appear anywhere in the body as lymphomas. Lymphocytes commonly reside in the conjunctiva and lacrimal glands. Orbital soft tissue is devoid of lymphocytes and lymph nodes. Although studies have argued that the orbit may be the primary site of malignant lymphoma, most lymphoproliferative diseases, including malignant lymphoma, can appear in one or both orbits without causing disease.
extraorbital. Intermediate- and high-grade lymphomas are rarer but more aggressive. About one-third of patients with lymphoma have extranodal disease. Orbital lymphoproliferation is usually extranodal or lymphoid because there are no lymph nodes in the orbit, lacrimal gland, eyelids, or conjunctiva. Patients with systemic lymphoma have about 1% orbital lymphoproliferation, but 30 to 40% of patients with lymphoma originating in the orbit never develop extraorbital manifestations on long-term follow-up. These lesions must be distinguished from inflammatory pseudotumor, which is sometimes difficult to distinguish. Spontaneous inflammation can affect any orbital structure, and is acute and painful. Inflammatory cells often incompletely infiltrate the orbital fat, lacrimal gland, and extraocular muscles. Acute or chronic inflammatory pseudotumor variants rarely progress to malignant lymphoma. According to the histopathological classification of non-Hodgkin's lymphoma, non-Hodgkin's lymphoma is divided into three main types with the following 5-year survival rates: low malignancy (5-year survival rate is 50-70%), intermediate malignancy (35-45%), and high malignancy (23-32%). The prognosis of patients with small cell lymphoma is similar to that of patients with polyclonal lymphoproliferative neoplasms. After 5 years of follow-up, about 15-25% of reactive lymphoid hyperplasia can transform into systemic lymphoma and the mortality rate is 6%, about 40% of atypical lymphoid hyperplasia can transform into systemic lymphoma and the mortality rate is 19%, about 75% of small cell lymphoma and 32% of atypical lymphoma originating from the orbit remain in the orbit. Patients with low-grade lymphoma have a survival of 5 to 7 years, which is better than that of similarly graded lymphomas at extramedullary sites.
other lymph nodes.51
1.2. Treatment of lacrimal gland tumors
Lacrimal gland tumors are very diverse in morphology and have many treatment options, depending on each specific case. Preoperative clinical and computed tomography evaluation is very important because if it is a benign mixed lacrimal gland tumor, biopsy is contraindicated because incomplete tumor excision will seed tumor cells leading to a high risk of recurrence. 12,52 In cases of acute inflammation that has just progressed within a few days, biopsy should not be performed, steroids should be used to reduce inflammation. Patients suspected of having a benign mixed lacrimal gland tumor with a long medical history, a lacrimal gland mass with a shell, round or oval shape should have both removed.
cortex-preserving mass through osteotomy. In case of suspected carcinoma, biopsy for definitive diagnosis followed by radical surgery to remove the tumor including soft tissue and bone. Currently, the treatment regimen for lacrimal gland cancer is eye-preserving surgery combined with radiotherapy and chemotherapy. Based on research results, eye-preserving surgery gives a good local control rate and is less affected by radiation toxicity. Intra-arterial chemotherapy or intravenous chemotherapy can reduce tumor size and achieve good results when combined with conservative surgery. However, the survival rate when treated with adjuvant chemotherapy has not been proven. Radiotherapy techniques such as proton radiotherapy can increase treatment effectiveness and have less toxicity to neighboring tissues such as the brain and eyeball. Targeted therapy studies targeting oncogenes applied to adenoid cystic carcinoma are especially valuable for recurrent or metastatic cancers from other locations. For lymphoma, a large enough tumor is biopsied through the eyelid, followed by postoperative radiotherapy to treat the remaining tumor. In cases of sarcoidosis or chronic inflammation, a trans-eyelid biopsy is required after systemic steroids. The basis of treatment for benign and malignant lymphoid lesions of the lacrimal gland is not surgery but a combination of multiple modalities of chemotherapy and radiotherapy. The surgical indication for lymphoma is surgery for the purpose of biopsy (a small piece of the tumor can be biopsied or the entire tumor can be removed as much as possible - both for the purpose of surgical removal of the tumor and for the purpose of biopsy for histopathology) to confirm the diagnosis, then choose the appropriate treatment method (chemotherapy or local radiotherapy).
1.2.1. Treatment of benign mixed lacrimal gland tumors
Indications and treatment methods : Treatment of benign mixed lacrimal gland tumors is mainly complete tumor excision, removing the entire tumor shell. Eyelid lobe tumors are indicated for complete excision through the eyelid crease. Orbital lobe tumors are indicated for complete excision through the lateral orbital osteotomy.
Contraindications : Do not biopsy to avoid tumor recurrence because incomplete tumor removal will spread tumor cells.
|
Maybe you are interested!
-
 Study on Some Clinical and Paraclinical Features of Appendiceal Abscess
Study on Some Clinical and Paraclinical Features of Appendiceal Abscess -
 Features of Verifying Conditions for Enforcement of Civil Judgments
Features of Verifying Conditions for Enforcement of Civil Judgments -
 Mapreduce And Hdfs (Optimal Features Of Mapreduce When Combined With Hdfs):hdfs Is Just A Distributed File System With Management Mechanisms Inside It.
Mapreduce And Hdfs (Optimal Features Of Mapreduce When Combined With Hdfs):hdfs Is Just A Distributed File System With Management Mechanisms Inside It. -
 Natural Features, Flood Control and Drainage Dyke System of the Study Area
Natural Features, Flood Control and Drainage Dyke System of the Study Area -
 Some Basic Features About Binh Gia District - Lang Son Province
Some Basic Features About Binh Gia District - Lang Son Province
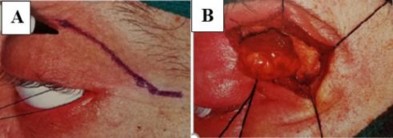
Figure 1.13. Surgical resection of mixed lacrimal gland tumor
A. Skin incision to remove tumor. B. Tumor during surgery. C. Gross image of tumor with capsule, bright yellow color, many small lobes
Source: Andreasen et al. (2016)53
Treatment results: Most mixed lacrimal tumors were completely removed en bloc, with no recurrence after treatment. Perez et al. (2006) studied lacrimal epithelial tumors and found that all benign mixed lacrimal tumors were completely removed en bloc, with only 1 patient undergoing orbital enucleation in 1974. No tumors recurred after treatment. Alkatan et al. (2014) stated that benign mixed lacrimal tumors are the most common type of benign epithelial tumor, accurately diagnosed and treated with the least risk of local recurrence. 54Overall, in benign mixed lacrimal gland tumors, the 15-year recurrence rate is less than 3% if the tumor is completely removed at the time of initial surgery,
32% if the tumor is biopsied for removal. Despite follow-up for recurrence, the 15-year survival rate is almost 100%. Long-standing, recurrent, and incompletely removed tumors may undergo malignant transformation. Malignant transformation is estimated to be 10% 20 years after initial treatment and 20% 30 years. Shields et al (2004) reported a median time to malignant transformation of 60 years.55According to Rose et al. (1992), to reduce the risk of recurrence and malignancy, mixed lacrimal gland tumors should be completely resected without biopsy.28
1.2.2. Treatment of lacrimal gland carcinoma
Adenoid lacrimal gland carcinoma is the most common malignant carcinoma of the lacrimal gland and is rare, accounting for only 1.6% of orbital tumors. The tumor grows slowly and often recurs despite treatment. The goal of lacrimal gland carcinoma treatment is local control and prevention of distant metastasis.
Indications and treatment : Appropriate treatment for lacrimal gland carcinoma is controversial. Historically, orbital debridement was the most commonly used surgical treatment for adenoid cystic carcinoma because the tumor was not encapsulated and the tumor often infiltrated the surrounding soft tissue. Orbital debridement combined with orbital bone resection is controversial if it is applied to all patients with malignant lacrimal gland carcinoma because of the survival benefit. In addition, some authors have suggested that removal of the orbital bone wall may cause the dissemination of residual tumor cells or peripheral tumor cells to the skull base. Orbital debridement involves the removal of the entire eyelid, conjunctiva, globe, optic nerve, extraocular muscles, lacrimal gland, and orbital fat. There are two techniques for orbital debridement: total eyelid resection and eyelid-preserving debridement. However, orbital debridement does not prevent recurrence or death. Later, the concept of globe-sparing surgery combined with radiotherapy allowed local control, vision preservation and minimal damage to the ocular surface. Postoperative adjuvant radiotherapy plays a key role in local control of lacrimal gland carcinoma, and is an important step in the treatment regimen for the management of lacrimal gland carcinoma, especially histological types with a tendency to perineural invasion such as adenoid cystic carcinoma. Radiotherapy is recommended for all malignant epithelial tumors and in cases of incomplete surgical resection, regional lymph node metastasis and extracapsular metastasis in non-adenoid cystic carcinoma. Proton radiotherapy is effective and has minimal effect on the brain and globe. During radiotherapy, the patient's anterior cornea is protected with a 12 mm oval corneal shield. This shield reduces the tumor dose by 15% and also reduces the effect on the macula and optic nerve. Monitor for complications such as cataracts, retinal damage, optic nerve damage, glaucoma, and damage to the remaining eye. Intra-arterial or intravenous chemotherapy to reduce tumor size is effective in combination with eye-sparing surgery, but the longevity benefit of adjuvant chemotherapy
has not been proven. Preoperative intra-arterial chemotherapy is only applicable to patients with intact lacrimal arteries.56Molecular biology studies have shown that cancer gene mutations account for a high proportion in lacrimal gland carcinoma, suggesting that targeted cancer gene therapy may be applicable to cases of metastatic or recurrent cancer.57
Treatment results: In some documents of Wright et al. (1992), patient survival rate was not related to orbital bone resection. 10In carcinoma, tumor recurrence in soft tissue or bone near the primary tumor site, lymph node metastasis or distant metastasis occurs less frequently and later. Statistical analysis shows that the risk
adenoid cystic carcinoma recurs many years after treatment. The recurrence rate of adenoid cystic carcinoma is more common in the basal cell type. Orbital debulking does not reduce the recurrence rate of adenoid cystic carcinoma.10 Of the 7 patients with adenoid cystic carcinoma treated at the University of Texas Anderson Cancer Center who underwent orbital debulking, orbital osteotomy, and postoperative radiation therapy, 5 patients developed distant metastases and died within 12 to 32 months after surgery. This result shows that the management of adenoid cystic carcinoma is very positive.
Although extensive surgery can control the local spread of the tumor, it does not reduce the risk of distant metastasis and does not improve mortality. Gensheimer et al (2013) described 11 patients with adenoid cystic carcinoma treated with neutron radiotherapy, of whom 4 patients underwent orbital debulking and 5 patients underwent eye-sparing followed by adjuvant neutron radiotherapy. The results were that 6/11 (54.5%) patients died at a mean follow-up of 6.25 years, 3/6 of these patients had local recurrence and 4 patients had distant metastasis. Overall, the 5-year local control rate was 80%, and in most cases, visual function was restored.
not well preserved.58
| |
C | D |
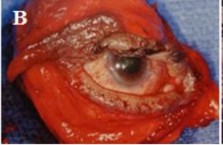
Figure 1.14. Surgical resection of adenoid cystic carcinoma
A. Surgical removal of the tumor, preserving the eyeball through the bone resection. B. Orbital tissue dredging model. C. Local radiotherapy, suitably designed Iodine-125 radiation plate placed above the outer orbit. D. I-125 active radiation plate and gold plate placed on the protective sclera
eyeball with radiation therapy
Source: Rootman et al. (2003)59
Complications after treatment : Radiation therapy can cause cataracts, damage to the retina, optic nerve, glaucoma and affect the remaining eye.
Since the 1930s, radiotherapy alone has been used to treat lacrimal gland tumors. In the following years, radiotherapy alone was replaced by radical orbital enucleation to reduce the rate of local recurrence and prolong life.60Reese et al. (1964) suggested that when carcinoma infiltrates bone, it will cause frequent tumor recurrence, so the initial surgery should be radical. They proposed resection of the outer wall and orbital rim, combined with orbital tissue dredging. There was only 1 patient.
10 years disease-free survival. This patient underwent curettage + bone resection, then radiation therapy, pathology showed that the resection had reached healthy tissue but the tumor had infiltrated the soft tissue of the orbit.61Henderson et al (1986) found that adenoid cystic carcinoma is the most common and most malignant type of lacrimal gland tumor. If we can find a way to treat adenoid cystic carcinoma, the treatment of other malignant lacrimal gland tumors will become much easier. Carcinoma
Cystic adenoma is also the most malignant primary tumor of the orbit. Radical bone resection should only be applied to cases of recurrent tumors, often tumors that slowly infiltrate with each surgery. Radical bone resection carries a high risk of sepsis, meningitis, and death. 62 In the following decades, the treatment of malignant lacrimal gland tumors has made significant progress. 21,63,64 Polito et al. (1993) pointed out the disadvantages of orbital tissue curettage, especially related to treatment results. 20,63 Meldrum et al. (1998) first reported the use of neoadjuvant chemotherapy in 2 patients with lacrimal gland carcinoma. The treatment regimen included intravenous Cisplatin and Doxorubicin, followed by orbital tissue curettage and orbital irradiation, and postoperative adjuvant chemotherapy was continued to enhance intravenous Cisplatin and Doxorubicin. 65 According to Esmaeli et al. (2004), most patients underwent radical surgery and significantly reduced recurrence. 66 Of the 6 patients who underwent orbital debridement with bone resection, 4 had clinical and histopathological evidence of bone, while 2 had no radiographic, clinical, or histopathological evidence of bone. These 2 patients subsequently underwent further bone resection to reduce the risk of future local recurrence. In the study by Perez et al. (2006), 4 cases of adenoid cystic carcinoma remained free of recurrence after 14, 27, 67, and 171 months, respectively, since treatment. There were 5 cases of local recurrence with or without distant metastases (lung, bone, brain), and all 5 died of the disease within a median of 77.8 months after treatment. There was 1 patient