Figure 1.1. Anatomy of the pancreas and islets of Langerhans 3
Figure 1.2. Pathogenesis of chronic pancreatitis 11
Figure 1.3. Progression of chronic pancreatitis 12
Figure 1.4. Pancreatic lesions on computed tomography 18
Maybe you are interested!
-
 Research on treatment of rotator cuff tears using modified Mason-Allen tendon endoscopic suturing technique and creating micro-damage at the attachment area - 2
Research on treatment of rotator cuff tears using modified Mason-Allen tendon endoscopic suturing technique and creating micro-damage at the attachment area - 2 -
 Research on diagnosis and endoscopic surgical treatment of benign adrenal tumors at Viet Duc Hospital in the period 1998 - 2005 - 20
Research on diagnosis and endoscopic surgical treatment of benign adrenal tumors at Viet Duc Hospital in the period 1998 - 2005 - 20 -
 Research on the application of smartphone utility software to evaluate traffic noise and road surface iri index - 14
Research on the application of smartphone utility software to evaluate traffic noise and road surface iri index - 14 -
 Research on the application of smartphone utility software to evaluate traffic noise and road surface iri index - 15
Research on the application of smartphone utility software to evaluate traffic noise and road surface iri index - 15 -
 Research on carbonization of agricultural by-products of coffee bean hulls and corn cobs by hydrothermal carbonization method, application as adsorbent and catalyst materials - 14
Research on carbonization of agricultural by-products of coffee bean hulls and corn cobs by hydrothermal carbonization method, application as adsorbent and catalyst materials - 14
Figure 1.5. Endoscopic ultrasound probe with 24 horizontal scanning
Figure 1.6. Endoscopic ultrasound probe with 25 vertical scanning
Figure 1.7. Clinical progression of chronic pancreatitis 31
Figure 2.1. Endoscopic ultrasound equipment at the Digestive - Endoscopy Center, Hue University of Medicine and Pharmacy Hospital. 46
Figure 2.2. Endoscopic ultrasound approaches to lesions 46
Figure 2.3. Pancreatic examination sites 47
Figure 2.4. Position of doctor and patient 48
Figure 2.5. Examination of the pancreas at the stomach position 49
Figure 2.6. Examination of the pancreas at the duodenal bulb 49
Figure 2.7. Examination of the pancreas at the D2 duodenum segment 51
Figure 2.8. Images of chronic pancreatitis on endoscopic ultrasound 54
Figure 3.1. Distribution according to history related to chronic pancreatitis 58
Figure 3.2. Pain level 63
Figure 3.3. Diabetes 64
Figure 3.4. Diagnosis of chronic pancreatitis according to Rosemont criteria 64
Figure 3.5. Value of endoscopic ultrasound in diagnosing early stage chronic pancreatitis 66
Figure 3.6. Complications of chronic pancreatitis 71
PROBLEM STATEMENT
Chronic pancreatitis is a disease characterized by inflammation and fibrosis of the pancreatic parenchyma, causing pancreatic duct dilatation, pancreatic duct stones or pancreatic calcification accompanied by endocrine and exocrine dysfunction [75], [88]. Chronic pancreatitis is increasingly common in clinical practice, with an annual incidence of about 5-14/100,000 people and a prevalence of about 30-50/100,000 people, varying between regions in the world [75]. According to Masamune's study on the epidemiology of early-stage chronic pancreatitis in Japan, the prevalence was 4.2/100,000 people and the incidence was 1/100,000 people [90]. The most dangerous complication of chronic pancreatitis is pancreatic cancer, with a 5-year survival rate of pancreatic cancer of about 7.8% [74]. The gold standard for diagnosing chronic pancreatitis remains histopathology, but pancreatic biopsy for diagnosis is not feasible clinically due to procedural complications. Recently, imaging tests such as ultrasound and computed tomography play an important role in diagnosis but have certain limitations. According to the American Pancreatic Association, computed tomography is valuable in diagnosing chronic pancreatitis in the late stage but is limited in diagnosing chronic pancreatitis in the early stage (moderate recommendation/moderate evidence) [33].
Endoscopic ultrasound has the advantage of high frequency, almost direct access to the pancreas, limiting fat tissue and gas in the digestive tract, so it can detect small changes in the parenchyma and pancreatic duct, in addition, it can also biopsy tissue samples in cases of pseudotumor chronic pancreatitis, so it has high value in diagnosing chronic pancreatitis and early stage chronic pancreatitis [61], [141]. Studies have demonstrated the correlation between criteria for diagnosing chronic pancreatitis on endoscopic ultrasound and histopathology [101], [123]. Currently, the diagnosis of chronic pancreatitis on endoscopic ultrasound is based on 2 criteria: the conventional criteria and the Rosemont criteria [104]. The conventional criteria include 9 criteria for pancreatic damage without distinguishing between the main and secondary criteria, so the accuracy of diagnosing chronic pancreatitis varies according to the number of signs of damage applied for diagnosis [123]. The Rosemont criteria are
More updated criteria with 11 pancreatic injury criteria divided into main criteria and secondary criteria help to accurately diagnose chronic pancreatitis or suspected chronic pancreatitis [31], [37].
Early diagnosis of chronic pancreatitis, especially detecting early-stage chronic pancreatitis, is very important to help limit damage to pancreatic stones, dilation of the main pancreatic duct, atrophy of the pancreas and complications of chronic pancreatitis [136], [142]. Early-stage chronic pancreatitis is the pivotal stage in the progression to chronic pancreatitis, an important stage if the patient is diagnosed early and risk factors are limited, there is a possibility of recovery [134]. The Japan Pancreatic Society published the criteria for diagnosing early-stage chronic pancreatitis in 2010, which is the first criterion for diagnosing early-stage chronic pancreatitis in the world based on clinical symptoms, biochemical tests, risk factors and small changes in the pancreas on imaging [116].
Currently, there has not been a complete study in the country on the role of endoscopic ultrasound in diagnosing chronic pancreatitis, especially in diagnosing early stage chronic pancreatitis. Therefore, we conducted the project: "Research on the application of endoscopic ultrasound in diagnosing chronic pancreatitis" with the following two objectives:
- Survey of endoscopic ultrasound characteristics in patients with chronic pancreatitis according to Rosemont criteria and early stage chronic pancreatitis according to Japanese Pancreatic Society criteria.
- Evaluate the relationship between some features on endoscopic ultrasound with clinical features, biochemical tests and computed tomography in patients with chronic pancreatitis.
Chapter 1
DOCUMENT OVERVIEW
1.1. ANATOMY, PHYSIOLOGY AND PATHOLOGY OF THE PANCREAT
1.1.1. Pancreatic anatomy
The pancreas is a gland in the digestive system that has both endocrine and exocrine functions. Exocrine function: secretes trypsin, amylase, lipase enzymes to digest food. Endocrine function: secretes insulin and glucagon to regulate blood sugar.
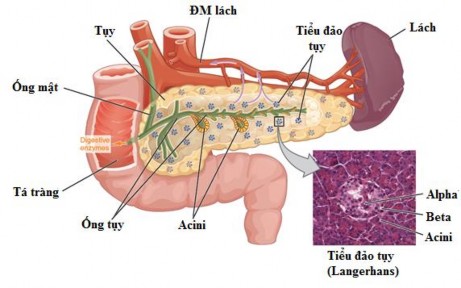
Figure 1.1. Anatomy of the pancreas and islets of Langerhans
(Source: Gordon Betts J, Anatomy & Physiology. OpenStax CNX, 2013) [51]
Location and external appearance of the pancreas
The pancreas is an organ located deep in the abdominal cavity, behind the peritoneum, soft in density, pinkish-gray in color, about 12 - 15 cm long, weighing about 80 grams. The pancreas goes from D2 duodenum, tilting upward to the left, lying horizontally in front of the lumbar spine L1 - L3, behind the stomach, all the way to the end of the splenic hilum. Most of it is in the upper layer of the transverse colon mesentery and a small part is in the lower layer of the transverse colon mesentery [1].
The pancreas is divided into four parts: head, neck, body and tail.
Pancreatic head: 3 cm thick, 7 cm high, 4 cm long, square with duodenum surrounding it, below the pancreatic head there is a hook, between the pancreatic head and the pancreatic body there is a defect.
also known as the isthmus of the pancreas. The position of the head of the pancreas corresponds to the L2 lumbar vertebra in the middle or slightly to the right. The head of the pancreas is flat, with two front and back surfaces suspended from the liver and duodenum by the hepatoduodenal ligament. The hepatoduodenal ligament is the boundary between the head and neck of the pancreas.
Pancreatic neck: 2 cm long, 3 cm high, 3 cm thick, usually located in front of the L1 lumbar vertebra, between the superior and inferior notches. The anterior part of the pancreatic neck is partially covered by the pylorus, behind is the portal vein formed by the confluence of the superior mesenteric vein and the trunk of the splenic vein.
Pancreatic body: 10 cm long, 4 cm high, 3 cm thick, triangular prism shape, lying diagonally from right to left at the level of the L1 lumbar vertebra. The anterior surface of the pancreatic body is in contact with the posterior leaflet of the posterior omentum and before that is the stomach. Posterior to the pancreatic body are the splenic vein, aorta and left renal vein.
Tail of the pancreas: continues with the body of the pancreas, can be long or short, round or flat depending on each individual, this is the most mobile part of the pancreas. The tail of the pancreas points towards the splenic hilum together with the splenic artery and the head of the splenic vein located in the splenopancreatic omentum [1].
Pancreatic ducts
Pancreatic juice is secreted through two main ducts: the main pancreatic duct (Wirsung duct) and the accessory pancreatic duct (Santorini duct).
Main pancreatic duct: runs along the axis of the pancreas from the tail of the pancreas to the body of the pancreas or slightly tilted upwards. At the isthmus of the pancreas, it curves downwards to the greater duodenal papilla and the common bile duct empties into the hepatopancreatic ampulla (ampulla of Vater). The main pancreatic duct receives the input of all the side branches, so its shape resembles a leaf.
Accessory pancreatic duct: separates from the main pancreatic duct at the neck of the pancreas and drains into the back of the duodenum at the small duodenal papilla, above the large duodenal papilla (2 cm above the Vater ampulla). The above anatomical images only account for 70 - 80% of cases, the remaining cases may include cases where the accessory pancreatic duct does not communicate with the duodenum or the accessory pancreatic duct is the main duct that drains into the duodenum. In cases where the main pancreatic duct drains pancreatic juice in
The head and hook empties into the greater papilla, a condition called pancreatic divisum, which is the result of a congenital anatomical abnormality and is also one of the causes of chronic pancreatitis [1].
1.1.2. Physiology of the pancreas
The pancreas is a digestive gland with two functions including endocrine and exocrine functions. Endocrine function: secretes insulin and glucagon to help regulate and metabolize sugar in the body. Exocrine function: secretes pancreatic juice containing trypsin, alpha chymotrypsin, amylase, lipase, small ducts secrete a large amount of bicarbonate solution into the Wirsung duct, then merges with the common bile duct at the Vater ampulla, then flows into the D2 segment of the duodenum through the Oddi sphincter.
Endocrine function: The pancreas secretes insulin and glucagon from alpha and beta cells in the islets of Langerhans. Insulin in the blood helps metabolize sugar. If for some reason, the pancreas does not secrete enough insulin to bring glucose into the cells, insufficient glycogen synthesis will lead to reduced carbohydrate metabolism, resulting in most of the blood glucose not being used and blood glucose levels increasing [9].
Exocrine function: Every day, the pancreas secretes about 1000ml of fluid through the pancreatic duct system into the ampulla of Vater. Pancreatic juice is an alkaline fluid containing a large amount of bicarbonate and digestive enzymes such as amylase, lipase, trypsin, chymotrypsin, carboxy polypeptidase, all three of these enzymes are secreted in the form of an inactive proenzyme, trypsinogen, chymotrypsinogen, procarboxypolypeptidase. When reaching the duodenum, some trypsinogen molecules are activated into trypsin and from there will reactivate other trypsinogens, then they continue to catalyze the activation of chymotrypsinogen into chymotrypsin and procarboxypeptidase into carboxypeptidase. Trypsin, chymotrypsin decomposes proteose peptones and polypeptide chains into smaller polypeptides. Carboxypolypeptidase cleaves amino acids from the carboxyl ends of polypeptide chains. Carbohydrate-digesting enzymes: alpha-enzymes
Pancreatic amylase digests both raw and cooked starch into maltose and a small amount of glucose polymers such as maltotriose and dextrin. Lipid-digesting enzymes: lipase is the most important neutral fat-digesting enzyme. Under the action of lipase, neutral fat is broken down into fatty acids, monoglycerides and a small amount of diglycerides. Pancreatic secretion is regulated by the nervous mechanism via the vagus nerve or enteric nervous system, and the humoral mechanism via the hormones: gastrin, cholecystokinin and secretin [9].
1.1.3. Pathological anatomy of chronic pancreatitis
1.1.3.1. General
Early stage: normal pancreas size.
Advanced stage: large, firm pancreas, edema due to acute inflammation, pancreatic duct may be normal or slightly dilated.
Late stage: The pancreas can shrink completely or partially, the pancreas is hard, there is fibrosis around the pancreas, the pancreatic duct can be dilated, in some cases it is narrowed or deformed. If there are pancreatic stones, they can be felt through the concave and convex surface of the pancreas, the pancreatic stones are opaque white, of different diameters, irregular in shape and hard. Pancreatic cysts can be felt to be soft, tense and there may be one or more cysts... The head, body and tail of the pancreas can be felt to be large and firm, easily mistaken for a pancreatic tumor, this is actually progressive fibrous tissue. Chronic pancreatitis is divided into 3 types: calcification, obstruction and fibrosis [9], [46].
1.1.3.2. Microscopic
Early stage: lesions are nodules affecting one or more lobes, partial or complete dilation of glandular follicles, fibrosis in and around the lobes, some pancreatic ducts are blocked by protein precipitation and calcium stones. Advanced stage: fibrosis throughout the glands, lobes are affected to varying degrees, pancreatic tissue is almost replaced by fibrous tissue [9], [46]. Studies have shown a correlation between pancreatic lesion criteria on endoscopic ultrasound in patients with chronic pancreatitis and histopathology [123].