work. We found that a significant proportion of patients with nasal valve stenosis were not given proper diagnosis and treatment.
There are many methods for diagnosing nasal congestion, including structural and functional examinations, objective or subjective from the patient [79],[83],[121]. Which method is necessary and sufficient to accurately diagnose the cause is a very important issue, helping doctors avoid ambiguity in diagnosis, come up with good surgical strategies and high treatment results.
Treatment of nasal congestion due to nasal valve stenosis is always a complicated problem, requiring the doctor to have both anatomical knowledge, a clear understanding of the physiological function of the nose, and the skills to perform surgery with high aesthetics. Currently, nasal valve correction with autologous cartilage is considered the optimal choice, with a very high treatment success rate from 83% to more than 90% depending on the author, the patient is no longer stuffy and the surgery is safe [8], [30], [70], [85].
There are 3 surgical approaches for nasal valve correction: closed surgical approach, closed surgical approach combined with endoscopic approach and open surgical approach. Each surgical approach has its own advantages and limitations, the indications depend on the abnormality of the nasal valve area and the type of graft needed. Closed surgical approach has the advantage of avoiding the risk of unsightly scarring of the external nose area but has many limitations: it can only intervene in a narrow area, cannot comprehensively assess the actual abnormalities of the nasal valve area, cannot combine many types of grafts if needed, difficulty in surgical manipulation & graft fixation and has the risk of creating adhesive scars in the nasal cavity [27],[31],[100]. Closed incision combined with endoscopy has the advantage of more clearly observing the structures that need intervention and avoiding the risk of bad scars affecting aesthetics, however, there are also limitations such as: expensive endoscopic equipment that not all medical facilities can equip, surgeons must be trained for a long time and systematically, surgery can only intervene in a limited area, cannot comprehensively assess abnormalities in the nasal valve area in reality, cannot coordinate many
Maybe you are interested!
-
 Research on treatment of rotator cuff tears using modified Mason-Allen tendon endoscopic suturing technique and creating micro-damage at the attachment area - 2
Research on treatment of rotator cuff tears using modified Mason-Allen tendon endoscopic suturing technique and creating micro-damage at the attachment area - 2 -
 Research on the treatment of seafood wastewater by electrocoagulation method combined with USBF - 19 tank
Research on the treatment of seafood wastewater by electrocoagulation method combined with USBF - 19 tank -
 Evaluation of the effectiveness of selective tibial nerve resection in the treatment of lower limb muscle spasticity sequelae - 19
Evaluation of the effectiveness of selective tibial nerve resection in the treatment of lower limb muscle spasticity sequelae - 19 -
 Studies on Leakage Water Treatment by Ozone in Vietnam
Studies on Leakage Water Treatment by Ozone in Vietnam -
 Follow-up Table of Patients Maintaining ARV Treatment After 12 Months
Follow-up Table of Patients Maintaining ARV Treatment After 12 Months
type of graft if needed, difficulty in surgical manipulation and graft fixation [26],[50],[100]. That is also the reason why today many authors have chosen the open incision in nasal valve correction and achieved a very high success rate. The disadvantage of the open incision is that it intervenes in the entire structure of the nose - nasal valve, which may have the risk of bad scarring, but it has outstanding advantages because: it can specifically assess abnormal structures, comprehensively correct the nasal valve, easy to fix, can combine many types of grafts at the same time, ensuring improvement in both nasal function and aesthetics, does not require expensive equipment and can be performed at any medical facility [7],[8],[70],[50],[84],[85],[101]. We decided to choose the open approach in nasal valve correction because this approach is most suitable for our patient, helps to resolve the nasal valve abnormalities and has been proven to be effective, stable and safe.
Nasal valve correction in Vietnamese patients must certainly have differences compared to published studies in the world because we have different characteristics in the physiological structure of the nose-nasal valve and the causes of the disease that we encounter every day in clinical practice.
We conducted the thesis: " Nasal valve correction through open surgery to treat nasal congestion " with the following research objectives:
1. Develop a technical process for nasal valve correction through open surgery, including the technique of using improved L-shaped grafts.
2. Evaluate the effectiveness of treatment of internal nasal valve stenosis through changes in clinical and paraclinical values compared before and after surgery.
3. Evaluate the stability of surgery after 6 months.
4. Evaluation of the safety of open nasal valve repair surgery.
Chapter 1
DOCUMENT OVERVIEW
1.1 ANATOMY AND PHYSIOLOGY OF THE NASAL VALVE AREA
1.1.1 Anatomy and physiology
When we breathe, the airways create resistance to help the incoming air to be channeled, warmed, moistened, and filtered of harmful agents. The nose is responsible for creating two-thirds of the airways' resistance. Most of this resistance is created in the anterior part of the nose, called the nasal valve [13].
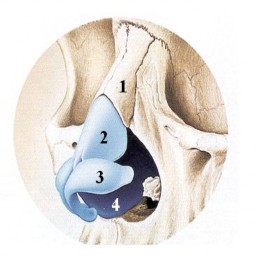
1. Nasal bone
2. Upper nasal cartilage
3. Nasal cartilage
4. Septal cartilage (quadrilateral cartilage)
Figure 1.1 Bone-cartilage structure of the nose
“Source: John S. Rhee, 2010” [54]
The anatomical structure of the nasal valve was first described by Mink [72] in 1903 and defined by Bridger [13] as that part of the nasal space bounded by the opening angle between the superior nasal cartilage and the septum. The angle between the superior nasal cartilage and the septum is approximately 10 0 -15 0 . This angle is maintained by the relationship
The relationship between the septum, the lateral nasal cartilages and the attachment of the facial muscles.
The nasal valve consists of the internal nasal valve and the external nasal valve. The internal nasal valve is limited by the superior nasal cartilage (ULC), nasal septum, nasal floor, and inferior turbinate (Figures 1.2,1.3).
The external nasal valve is the outermost part of the internal nasal valve, bounded externally by the alar (LLC) and internally by the septum & columella [54], [55], [58].
Inner nasal valve
External nasal valve
Figure 1.2 Position of internal and external nasal valves
“Source: John S. Rhee, 2010” [54]
Nasal valve area
Inferior turbinate
Side of the nose
Partition
Inner nasal valve
Figure 1.3 Structures related to the internal nasal valve
“Source: John S. Rhee, 2010” [54]
The medial nasal valve angle is the angle formed by the superior nasal cartilage and the septum [58],[84]. Narrowing of this angle is considered a common cause of nasal obstruction in Caucasian patients and requires rhinoplasty [85]. The medial nasal valve angle in Caucasians ranges from 10 0 -15 0 . The medial nasal valve angle in Asians ranges from 21.6 0 4.5 0 [79].
The nasal valve consists of the cartilage structures of the nose, the erectile tissues, mainly the inferior turbinate, which are responsible for regulating air through the nose. The nasal valve is the place with the highest nasal impedance because it is the narrowest part of the nose. The cross-sectional area through the nasal valve is between 55-85 mm 2 [37],[47]. According to Bernoulli's principle: when there is a change in pressure when a stream of solution (or gas) passes through a narrow place, the velocity of the stream of solution (or gas) when passing through the narrow place will increase, reducing the pressure in the area after the narrow place [25]. This explains the phenomenon
Lateral nasal wall collapse and nasal congestion in patients with nasal valve stenosis. Also due to the difficulty in passing through this nasal valve area, air velocity will decrease, ensuring the function of purifying, warming and humidifying the air.
1.1.2 Nasal valve stenosis and racial differences
The cause of nasal valve stenosis is very different in white Europeans and Americans and yellow Asians due to different anatomical structures.
White Europeans and Americans have a nose structure: developed nasal bone, high and neat nasal bridge, thin nasal skin and thick nasal cartilage, often with bone and cartilage overgrowth causing a bumpy nasal bridge, etc. Nasal valve angle is between 10 0 -15 0 .
In studies on European and American patients, nasal valve stenosis is the most common cause of nasal obstruction [85]. After rhinoplasty, nasal trauma, lateral nasal wall collapse, nasal tip prolapse, etc. are causes of nasal valve stenosis (Figures 1.4, 1.5, 1.6). In a study on 500 patients with chronic nasal obstruction, Elwany and Thab found that nasal valve stenosis occurred in 13% of patients.
cases of nasal obstruction [32]. Excessive rhinoplasty is the most common cause of nasal valve stenosis. Author Maurice M. Khosh et al. in a study of 53 patients showed that nasal valve stenosis due to excessive rhinoplasty was 79%, due to nasal trauma was 15% and congenital was 6% [70]. Author Constantian in a study of 100 patients with secondary rhinoplasty found that 50% of patients had external nasal valve stenosis and 64% had internal nasal valve stenosis [23].
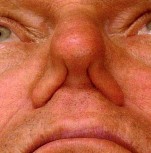
Figure 1.4 Bilateral nasal valve stenosis - Bilateral nasal wall collapse during inhalation
“Source: Charles G. Hurbis, 2006” [17]

Figure 1.5 Right nasal valve stenosis - Collapse of the right nasal wall during inhalation
“Source: Charles G. Hurbis, 2006” [17]
Figure 1.6 Nasal valve stenosis due to excessive rhinoplasty -
Inverted "V" shaped nose
“Source: Charles G. Hurbis, 2006” [17]
Asians with yellow skin have a nasal structure: the main nasal bone is underdeveloped, the bridge of the nose is low and wide, the nasal skin is thick but the nasal cartilage is thin, there is less nasal bridge hump, the internal nasal valve angle is larger and in the range of 21.6 0 4.5 0 [79]
There are not many studies and statistics on the rate of nasal valve stenosis as well as appropriate treatment methods in Asians. There are only studies describing the structure of the nasal valve [1] and the internal nasal valve angle indexes [79], or studies on nasal valve orthopedics in some typical cases by author Hong-Ryul Jin (Korea) [50].
In clinical practice, we encounter patients with nasal valve stenosis due to nasal trauma with the highest rate, followed by post-nasal surgery, congenital nasal valve stenosis, and nasal valve stenosis due to old age. (Figures 1.7, 1.8, 1.9, 1.10)
Figure 1.7 Post-traumatic nasal valve stenosis
Figure 1.8 Nasal valve stenosis due to aging - Collapse of the lateral nasal wall when inhaling
Figure 1.9 Congenital nasal valve stenosis
Figure 1.10 External nasal valve stenosis – image of nasal tip prolapse