- Level of consciousness assessed by Glasgow scale at admission
- Stroke severity is assessed by the NIHSS scale, which is a scale to assess the severity of neurological damage in ischemic stroke, with scores ranging from 0 to 42 points (Appendix C), the higher the score, the more severe the neurological damage. There is no specific cut-off point to distinguish between mild and severe patient groups, but clinical and research often use the cut-off point of 4 points or less as mild, 25 points or more as very severe, and the intermediate level can take the cut-off point of 15 (5-14 is moderate, 15-24 is severe).
- The damaged hemisphere, based mainly on clinical findings, confirmed by imaging, has two values: right hemisphere or left hemisphere.
- Classification of the cause of cerebral infarction according to TOAST [28]: includes five groups: cerebral infarction due to large artery atherosclerosis, due to embolism from the heart, due to small artery disease (lacunar infarction), due to other specified causes, and unknown causes. This classification has been widely popularized both in clinical practice and in clinical studies and trials on stroke. Determining the cause according to TOAST in our study was based on the following surveys: 12-lead electrocardiogram, echocardiography, extracranial carotid-vertebral duplex ultrasound, magnetic resonance angiography or computed tomography, and blood lipid tests, assessment of risk factors.
Maybe you are interested!
-
 Outcomes of Functional Recovery, Mortality, and Recurrence in Patients with Cerebral Infarction and Internal Carotid Artery Occlusion
Outcomes of Functional Recovery, Mortality, and Recurrence in Patients with Cerebral Infarction and Internal Carotid Artery Occlusion -
 Aspects of the Km Star Model Source: According to Nirmal Pal and Associates
Aspects of the Km Star Model Source: According to Nirmal Pal and Associates -
 Survey of prognostic factors of cerebral infarction due to internal carotid artery occlusion - 2
Survey of prognostic factors of cerebral infarction due to internal carotid artery occlusion - 2 -
 Stakeholders in Relationship with Investment Capital in Defense Economic Zones
Stakeholders in Relationship with Investment Capital in Defense Economic Zones -
 Objective Aspects of the Crime of Intentionally Causing Injury or Harm to the Health of Another Person
Objective Aspects of the Crime of Intentionally Causing Injury or Harm to the Health of Another Person
A patient is defined as having macrovascular disease if there is evidence of atherosclerosis in the carotid artery where the obstruction is located, and/or in other intracranial and extracranial arteries; the more severe the degree of atherosclerosis and stenosis, the higher the certainty of the diagnosis; and there is no cardiac source of embolism.
Cardiac embolism is defined if the patient does not have significant atherosclerosis in the occluded carotid artery, and is further defined if there is no atherosclerosis in other arteries, and there is a high-risk cardiac embolism source by definition, of which atrial fibrillation is the leading cause, but it can also be valvular heart disease, prosthetic valve, acute myocardial infarction, etc.
Patients were diagnosed with small vessel cerebral infarction when there were no lesions or lacunar brain lesions (<1.5 cm in diameter) in the deep regions or brainstem, clinical lacunar syndrome, no signs of cortical lesions, newly identified or known hypertension and/or diabetes.
Patients were classified as having unknown cause if no obvious cause was found, or if there was both large-vessel atherosclerosis and a cardiac source of embolism. Other causes were defined if there was sufficient evidence (e.g., arterial dissection seen on angiography and/or duplex ultrasound) and cerebral ischemia consistent with the abnormal artery.
The electrocardiogram is measured using a three- or six-lead electrocardiograph, measuring the standard 12 leads and measuring long DII if there is a suspected arrhythmia. The results are read by a cardiologist and recorded in the medical record.
Echocardiography is performed by cardiologists in the functional diagnostics department, the ultrasound machines used are GE, Aloka, Acuson CV70.
2.2.2.4. Imaging variables
Brain parenchymal imaging variables: ASPECTS score and Bang's infarct segmentation
Brain parenchyma images are examined by CT scan on Siemens Esprit VA-47C, Sensation 4, Presto, Biograph 64 machines, or by MRI on Avanto – MR B15 machine, the results are read by an imaging doctor assigned by the hospital's diagnostic imaging department.
- Brain lesions on CT scans are assessed using the ASPECTS scale. The ASPECTS scale scores based on the assessment of cerebral ischemic lesions in the perfusion area of the middle cerebral artery [37]. The perfusion area of the middle cerebral artery is divided into 10 regions (Figure 2.1) on cross-sections through the basal ganglia.
and slices immediately above the basal ganglia, including four deep regions: I (insular), C (caudate), IC (internal capsule), L (lenticular) and six superficial regions: M1, M2, M3 in slices through the basal ganglia, and M4, M5, M6 in slices close to the basal ganglia. If there is no lesion, the score will be 10, each area of cerebral infarction will be deducted one point, up to the most severe is 0 points when the entire middle cerebral artery perfusion area is damaged. The ASPECTS scale has been shown to have high inter-rater agreement and high reliability in disease prognosis [37], [107]
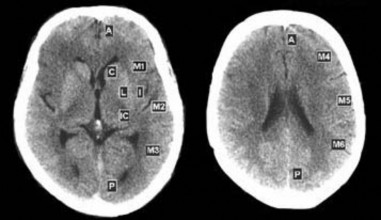
Figure 2.1. ASPECTS scoring partitions “Source: Pexman JHW, 2001” [107]
- Brain damage assessment on imaging according to the location and size of the lesion, briefly called Bang's (et al.) infarction classification [35]: in 2005, Bang and colleagues proposed a classification of brain damage according to the location and size of the cerebral infarction lesion, including six types (Figure 2.2).
(1) Lobar cerebral infarction in two or more segments of the middle cerebral artery perfusion territory
(2) Other cortical infarction: cortical infarction in 1 segment or in the cortical border area
(3) Small cortical infarction: multiple small cortical infarctions (<1cm) or single or multiple infarctions in the center of the semiovale
(4) Deep border zone infarction (multi-lobed chain lesions, located alone or connected to striatal lesions, located in the supraventricular or paraventricular regions)
(5) Small deep infarction
(6) Other deep infarcts: large infarcts in the corpus striatum (lesion)
>15mm), or additional lesions outside the striatum-internal capsule area.
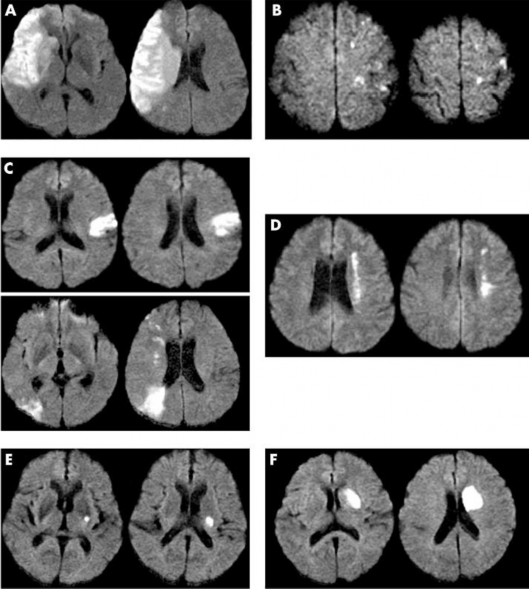
Figure 2.2. Brain lesion stratification by State. (A) Lobar infarction, (B) Small superficial infarction, (C) Other superficial infarction, (D) Deep border infarction, (E) Small deep infarction, and (F) Other deep infarction. “Source: State OY, 2005”[35]
Bang et al noted that this classification can help predict early functional outcome and recurrence in patients with infarction [35].
From this classification, we adjusted the names and order for easier use, including six types as follows:
(1) Small superficial infarction: multiple small infarctions in the cerebral cortex or single or multiple infarctions in the center of the semiovale.
(2) Small deep infarction.
(3) Monocortical infarction: monocortical infarction or cortical border zone infarction.
(4) Deep border infarction
(5) Large deep infarction: deep infarction >1.5cm in size or with infarction outside the lenticule area
(6) Extensive infarction (lobar): extensive infarction from two parts to the entire middle cerebral artery perfusion area (deep segment, superior superficial branch perfusion area, inferior superficial branch perfusion area).
Cerebrovascular imaging variables
- Carotid artery obstruction side: same value as the variable on the side of the damaged hemisphere, has two values: right side and left side
- Ipsilateral M1 middle cerebral artery status: reflects the residual perfusion of the middle cerebral artery on the same side as the occluded internal carotid artery, reflecting the effectiveness of collateral circulation. This variable has four values: normal, mild caliber reduction (<50% of the original caliber, compared to the original or to the contralateral M1), severe caliber reduction (50% or more), and complete loss of flow (total M1 or at any location of M1); A fifth value is not available, occurring in a small number of patients who are too ill at the outset to undergo intracranial angiography.
- Contralateral internal carotid artery status: to partly reflect the patient's carotid atherosclerosis status and is the basis of the main collateral supply to the brain. This variable has four values: normal, mild stenosis <50% diameter (ie ≥50% diameter), severe stenosis of 50% diameter or more, and complete occlusion.
Determine the status of collateral blood supply
- Collateral blood supply to the middle cerebral artery: determining the collateral blood supply through the anterior communicating artery, posterior communicating artery, or both, is assessed based on vascular imaging (CTA, MRA). Blood supply through the anterior communicating artery is determined when there is sufficient continuous vascular signal from the contralateral internal carotid artery, to the A1 segment of the contralateral anterior cerebral artery and good signal from the A2 segment of the ipsilateral anterior cerebral artery; at the same time, there is no continuous signal of the blood supply through the posterior communicating artery. Blood supply through the posterior communicating artery is determined when there is continuous vascular signal from the basilar artery, the P1 segment of the ipsilateral posterior cerebral artery, the ipsilateral posterior communicating artery, the A1 and A2 segments of the ipsilateral anterior cerebral artery; at the same time, there is no continuous signal of the collateral through the anterior communicating artery. Blood supply through both the anterior and posterior communicating arteries is determined when there is continuous vascular signal from both of the above pathways. In cases where the vascular signal of the ipsilateral anterior cerebral artery is seen but the blood supply through the two above routes is not seen, with or without recording the blood supply from another artery, we record the presence of collateral blood supply of unknown source.
- The collateral blood supply to the middle cerebral artery is determined similarly above. The collateral route through the anterior communicating artery starts from the contralateral internal carotid artery, reaches the contralateral A1 segment, via the anterior communicating artery (usually not seen on film) via the ipsilateral A1 segment, and reaches the ipsilateral M1 middle cerebral artery. The collateral route through the posterior communicating artery starts from the basilar artery, reaches the P1 segment of the artery
ipsilateral posterior cerebral artery, via the posterior communicating artery, to the terminal internal carotid artery and supplies the ipsilateral middle cerebral artery M1 segment.
Determine the mechanism of cerebral infarction
- The mechanism of cerebral infarction is determined relatively, based on the characteristics of brain damage, combined with the characteristics of cerebral vascular imaging, mainly the collateral status and the status of the ipsilateral M1 segment.
- In patients with internal carotid artery occlusion and infarction occurring in all or nearly all of its perfusion territory, or in the entire middle cerebral artery in the absence of collaterals through the circle of Willis, the mechanism is determined to be direct embolism due to the internal carotid artery occlusion.
- The remaining patients have infarcts that are part of the middle cerebral artery, or the anterior cerebral artery (rare), which are cases of internal carotid artery occlusion and some degree of collaterals, the infarct mechanism will be hemodynamic or embolization in a branch of the occluded carotid artery. The hemodynamic mechanism is determined when there is a lesion in the distal area - the border area, accompanied by a signal decrease or localized stenosis in the ipsilateral M1 segment. The embolization mechanism is determined when there is occlusion of a branch of the artery and infarction in its perfusion area, or infarction in a branch perfusion area of the middle cerebral artery (or anterior cerebral artery) and no signal decrease in perfusion (reduced common diameter, decreased contrast signal) or localized stenosis in the proximal large arterial segments. Cases classified as mixed mechanism are when both groups of characteristics coexist, while cases with unknown mechanism are when none of the above two groups are seen.
2.2.2.5. Paraclinical variables
- Blood sugar on admission, in mg/dL
- Ionogram: Na, K, Ca, Cl, in mEq/L, first result taken upon admission
- Blood lipid profile: Total cholesterol, LDL cholesterol, HDL cholesterol, Triglyceride, in mg/dL, first results taken upon admission
- BUN, blood creatinine, in mg/dL, first result taken upon admission
- Electrocardiography, echocardiography, and carotid duplex ultrasound were performed in all patients and the results were recorded, but mainly served to determine the value of other variables such as cardiovascular risk factors (coronary artery disease, atrial fibrillation, etc.) or determine the cause (TOAST classification), screen for arterial occlusion, and the status of the contralateral carotid artery.
2.2.2.6. Antithrombotic drug treatment variables
- Record the type of antithrombotic medication the patient used during the hospital stay up to the first visit after 30 days, including aspirin use, clopidogrel use, and oral anticoagulant use (sintrom).
- Subsequent follow-up visits are only recorded for reference and not analyzed, due to the inability to closely control the patient's long-term use of medication.
2.2.2.7. Outcome variables
- Recurrent cerebral infarction: new focal neurological signs appear, and/or there is imaging evidence of a new cerebral infarction lesion.
- The level of functional recovery was assessed by the modified Rankin scale (mRS) (appendix), which includes seven scores: 0 - no symptoms; 1 - mild symptoms but no functional impact, able to perform all normal tasks and activities; 2 - mild functional loss, unable to perform all previous activities, but still able to take care of oneself without assistance; 3 - moderate disability, requiring some assistance, but still able to walk without assistance; 4 - moderate disability, unable to walk without assistance and unable to care for bodily needs without assistance; 5 - severe disability, bedridden, loss of bladder and bowel control and requiring constant nursing care; and 6 - death. In this study, because brain damage in internal carotid artery occlusion is often severe, the possibility of complete recovery and independence is low, so we did not use a cutoff point of 2 as in other studies.