3.4.3.3. Cox regression analysis for the composite event of all-cause mortality or readmission 46
CHAPTER 4: DISCUSSION 47
4.1. General characteristics of research subjects 47
4.1.1. Clinical features 47
4.1.2. Paraclinical characteristics 49
Maybe you are interested!
-

 Testing the Relationship Between Patient Age and Erectile Dysfunction
Testing the Relationship Between Patient Age and Erectile Dysfunction -
 The relationship between travel motivation, destination image and destination choice - A case study of Binh Dinh province tourism destination - 1
The relationship between travel motivation, destination image and destination choice - A case study of Binh Dinh province tourism destination - 1 -
 The Impact of Investor Protection Rights on the Relationship Between Liquidity and Firm Value
The Impact of Investor Protection Rights on the Relationship Between Liquidity and Firm Value -
 Relationship Between Research Variables in the Model
Relationship Between Research Variables in the Model -
 Customer relationship management in competitive strategy and lessons for Vietnamese enterprises - 13
Customer relationship management in competitive strategy and lessons for Vietnamese enterprises - 13
4.2. Characteristics of BMI index in patients with chronic heart failure 51
4.3. Relationship between BMI and clinical and paraclinical characteristics in patients with chronic heart failure 52
4.4. Association between BMI and outcomes in patients with heart failure 53
CONCLUSION 58
PROPOSAL 60
APPENDIX
PROBLEM STATEMENT
Heart failure is one of the diseases with the highest morbidity and mortality rates in the world. According to the results of the Global Burden of Disease, Injuries, and Risk Factors (GBD) 2017 study conducted by the Institute for Health Metrics and Evaluation (IHME), the number of heart failure patients worldwide nearly doubled from 33.5 million in 1990 to 64.3 million in 2017 [1]. A meta-analysis of 1.5 million heart failure patients estimated the 1-, 2-, 5-, and 10-year survival rates to be 87%, 73%, 57%, and 35%, respectively, and the overall 1-year survival rate for people < 65 years of age was 91.5% compared with 83.3% for people ≥ 75 years of age [2]. In the US, there are currently about 5.7 million people with heart failure, and the worrying prediction is that by 2030 there will be more than 8 million people with this disease, the prevalence rate will increase to 46% [3]. In Vietnam, there has been no major study to assess the situation of heart failure in the community. Statistics in 1991, at the Vietnam Heart Institute, the number of patients with heart failure accounted for 59% of the total number of hospitalized patients and 48% of the total number of patients who died. In 2000, the number of patients with heart failure requiring treatment at the Heart Institute was also up to 56.6% [4, 5]. According to statistics in 2016 at Hanoi Heart Hospital, the rate of hospitalization for heart failure accounted for 15% of the total number of hospitalizations [6]. Although there has been much progress in the diagnosis and treatment of heart failure today, heart failure is still a burden for all of humanity, the mortality rate in this group of patients remains high.
Obesity is known to be a significant risk factor for cardiovascular disease as well as the progression of heart failure. In 2005, the world had approximately 1.3 billion overweight and obese people, accounting for more than 30.0% of the world's adult population, and this value is estimated to nearly double by 2030. Although overweight and obesity are more common in countries with developed economies, developing countries have been projected to have a much larger increase in the number of overweight and obese people between 2005 and 2030 [7]. According to the 2021 statistics from the World Population Assessment, Vietnam still has the lowest obesity rate at 2.1% [8]. However, Vietnam had the highest obesity growth rate in Southeast Asia from 2010 to 2014. In 5 years, Vietnam's obesity rate increased to 38% [9]. The results of the 2019-2020 General Nutrition Survey recently published by the National Institute of Nutrition of Vietnam showed that the rate of overweight and obesity increased from 8.5% in 2010 to 19.0% in 2020, of which the rate of overweight and obesity in urban areas was 26.8%, in rural areas was 18.3% and in mountainous areas was 6.9% [10].
Overweight and obesity can lead to heart failure through several direct and indirect pathways. Higher body mass index (BMI) leads to changes in total body hemodynamics leading to increased stroke volume, cardiac output, and blood pressure. Adverse changes in cardiac hemodynamics and structural morphology have also been found in individuals with high BMI. According to the Framingham study, a one-unit increase in BMI increased the risk of heart failure by 5% in men and 7% in women. Higher BMI itself may be a strong risk factor for heart failure regardless of age, sex, and ethnicity. A 2002 report found that 32%–49% of people with heart failure were obese and 31–40% were overweight [11]. Because of the evidence that obesity is detrimental to cardiovascular health, weight loss is often recommended as a treatment goal for patients with heart failure and high BMI.
However, some recent studies have shown the “obesity paradox” in patients with chronic heart failure. After a meta-analysis including 28,209 heart failure patients (followed up for 2.7 years), it was shown that in overweight patients, the rate of all-cause mortality was 16% lower and the rate of cardiovascular mortality was 19% lower than in patients with normal BMI[12]. In addition, the obese group had a 33% and 40% lower rate of all-cause mortality and cardiovascular mortality, respectively, compared with the normal BMI group. Recent reports have also confirmed the obesity paradox in heart failure with preserved left ventricular ejection fraction as well as heart failure with reduced left ventricular ejection fraction. The underlying molecular mechanism by which obesity improves prognosis in patients with heart failure remains poorly understood[13].
In Vietnam, studies on this issue are limited, so we conducted a study: " The relationship between BMI index and prognosis of death and re-hospitalization in chronic heart failure patients treated as outpatients at the Vietnam Heart Institute " with two objectives:
1. Describe the general characteristics and BMI index in chronic heart failure patients treated as outpatients at the Vietnam Heart Institute, Bach Mai Hospital from 2018 - 2020
2. Initial investigation of the relationship between BMI and clinical and paraclinical characteristics and prognosis of death and rehospitalization in patients with chronic heart failure.
Keywords: chronic heart failure, body mass index (BMI), overweight and obesity, re-hospitalization, mortality,..
CHAPTER 1: OVERVIEW
1.1. Overview of chronic heart failure
1.1.1. Definition of heart failure and chronic heart failure
In 1980, cardiologist Eugene Braunwald defined: "Heart failure is a pathological condition, with abnormalities in heart function, not being able to pump enough blood to meet the metabolic needs of the tissue" [14].
Based on the recommendations of the European Society of Cardiology (ESC) 2013, the Vietnam Cardiovascular Association defines heart failure: "Heart failure is a complex clinical syndrome that results from physical damage or dysfunction of the heart, leading to the ventricles being unable to receive blood (diastolic heart failure) or eject blood (systolic heart failure)" [15].
However, the definitions of heart failure in clinical practice and in scientific research are considered difficult to standardize. Most agree that heart failure is a clinical syndrome, but the diagnostic criteria are not clear. Therefore, the World Cardiology Association has issued a common global definition of heart failure: “Heart failure is a clinical syndrome with the following currently or previously occurring:
- Symptoms and/or signs due to structural and/or functional cardiac abnormalities (defined by ejection fraction (EF) < 50%, abnormally enlarged chambers, E/E' > 15, moderate/severe ventricular hypertrophy, or moderate/severe valvular stenosis or regurgitation)
- And be certified by at least one of the following:
Increased natriuretic peptide concentration
Objective evidence of pulmonary or systemic congestion by diagnostic means, such as imaging (eg, by chest radiograph or increased ventricular filling pressures detected by echocardiography) or hemodynamic measurements (eg, right heart catheterization, pulmonary artery catheterization) at rest or with stimulation (eg, exercise)”
Such a definition is sufficiently comprehensive and practical to provide a basis for further classification and may include formal disease stages, with universal applicability, prognostic and therapeutic value, and acceptable sensitivity and specificity.
Most recently, the ESC issued its 2021 recommendations with a definition of heart failure that is not much different from the 2016 one: “Heart failure is not a single pathological diagnosis, but a clinical syndrome consisting of cardinal symptoms (e.g. dyspnea, leg edema, and fatigue) that may be accompanied by signs (e.g. jugular venous distention, pulmonary rales, and peripheral edema). It is due to structural and/or functional abnormalities of the heart that lead to increased intracardiac pressures and/or cardiac output imbalances at rest and/or during exercise” [16].
Chronic heart failure is a patient with heart failure for a relatively long time. If the patient's condition does not deteriorate for at least 1 month when treated, it is called stable. On the contrary, if the stable condition is lost, the patient will progress to decompensated chronic heart failure, this process can occur slowly or quickly, this is the cause of hospitalization and is a poor prognostic factor [17].
1.1.2. Epidemiology of chronic heart failure
1.1.1.1. Prevalence of heart failure
Results from the Global Burden of Disease, Injuries, and Risk Factors (GBD) 2017 study conducted by the Institute for Health Metrics and Evaluation (IHME) show that the number of patients with heart failure worldwide nearly doubled from 33.5 million in 1990 to 64.3 million in 2017 [1]. Age-standardized prevalence rates indicate that aging and population growth are responsible for most of the increase in prevalence. At the same time, heart failure is increasing in low, low-middle, and middle SDI (SDI - SociodeMographic Index) countries [18], driven by increases in risk factors such as hypertension, diabetes, obesity, smoking, and other unhealthy lifestyles [19].
In the United States, approximately 5.7 million people currently have heart failure, and it is alarmingly predicted that by 2030, more than 8 million people will have this disease, a prevalence rate that will increase to 46% [3]. Studies in Europe have a prevalence rate of approximately 3/1000 people/year, with an incidence rate of 5/1000 people in adults [16]. In Asia, data on the prevalence of heart failure show that the number is lower. In China, 500,000 new cases of heart failure are diagnosed each year, accounting for 0.9% [20], and in India, approximately 0.5–1.8 million new cases per year (rate of 0.05–0.17%) [21]. Recent data show that the prevalence of heart failure in Southeast Asia is similar to that in the world, with heart failure accounting for up to 20% of hospital admissions [6].
1.1.1.2. Mortality rate
Estimates of mortality from heart failure vary depending on study design, baseline risk of the population studied, criteria for assessing heart failure, and cut-off values for left ventricular ejection fraction. Death in heart failure is usually due to two main causes: pump failure and arrhythmias. Mortality in patients with heart failure is very high and increases with age. The Framingham study showed that the 1-year all-cause mortality rate of patients with heart failure was 57% in women and 64% in men, and the 5-year survival rate was 38% in women and 25% in men [22]. A meta-analysis of 1.5 million patients with heart failure estimated 1-, 2-, 5-, and 10-year survival rates of 87%, 73%, 57%, and 35%, respectively, and an overall 1-year survival rate of 91.5% in those <65 years of age compared with 83.3% in those ≥75 years of age [2]. The MAGGIC study pooled data from 31 observational studies and clinical trials, showing that patients with heart failure with preserved ejection fraction (HFpEF) had a 32% lower risk of death than patients with heart failure with reduced ejection fraction (HFrEF), and a 22% lower risk after excluding clinical trials [23].
1.1.1.3. Hospital readmission rate
Thanks to advances in treatment for heart failure, survival rates in heart failure patients have improved significantly. However, the rate of rehospitalization for heart failure remains high, with 30-day readmission rates ranging from 19% to 25% in a survey of approximately 26 million people with heart failure [24] . Older patients with heart failure are at higher risk of rehospitalization due to decline in physical function [25, 26] . According to Ishihara et al., heart failure patients who were rehospitalized within 3 months had higher all-cause and cardiovascular mortality rates [27]. In Southeast Asia, heart failure patients have a hospital stay of 5 to 9 days and a 30-day readmission rate of 7% to 17.6% [6].
In Vietnam, there has been no major study to assess the prevalence of heart failure in the community. At the Vietnam Heart Institute, in 1991, the number of patients with heart failure accounted for 59% of the total number of hospitalized patients and 48% of the total number of deaths. In 2000, the number of patients with heart failure requiring treatment at the Heart Institute was up to 56.6%. With a population of about 80 million people and a frequency of infection like Europe, it is estimated that our country has about 320,000 to 1.6 million people with heart failure requiring treatment [4, 5]. According to 2016 statistics at Hanoi Heart Hospital, the rate of hospitalization for heart failure accounted for 15% of the total number of hospitalizations [6].
1.1.3. Pathophysiology of heart failure
The origin of the symptoms of heart failure is still unclear. It may be from an initial event (myocardial infarction, myocarditis, volume overload, etc.) that causes myocardial damage, leading to increased pressure on the heart wall. This affects the heart's ability to pump blood to meet the body's oxygen needs, leading to a decrease in cardiac output. The body has some limited compensatory responses to circulatory failure, mainly vasoconstriction, sodium and water retention through neuroendocrine activation and cardiac reflex abnormalities (Figure 1.1). However, these adjustments to the state of reduced circulatory volume are poorly matched to the state of pump failure, and the increase in cardiac preload and afterload leads to worsening heart failure. This condition is also known as the "pathological spiral of heart failure" [28].
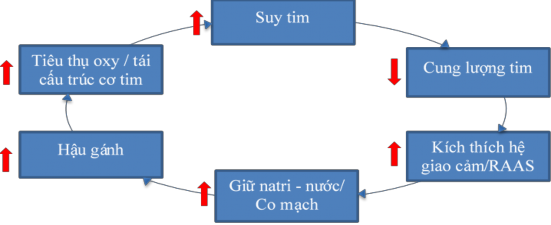
Figure 1.1. Pathological spiral of heart failure [28] .
When heart failure occurs, compensatory mechanisms play a very important role in maintaining stable cardiac output as well as circulatory system activity. Compensatory mechanisms include:
Compensatory mechanism in the heart:
Ventricular dilatation: Ventricular dilatation is the first adaptive mechanism to avoid excessive end-diastolic pressure of the ventricles. When the ventricles dilate, it will lengthen the myocardial fibers and according to Starling's law, it will increase the contractile force of the myocardial fibers if the contractile reserve is still present [5].
Ventricular hypertrophy: to maintain wall tension during ventricular dilation, the heart can adapt by increasing the thickness of the cardiac walls with or without chamber dilation, especially in cases of increased pressure in the cardiac chambers. However, it is eventually no longer appropriate because the hypertrophied myocardium exceeds the growth of the blood supply [5].
Adverse myocardial remodeling: Increased myocardial volume, mass, and apoptosis promote extensive myocardial remodeling to adapt to new conditions (Starling and Laplace laws). This is not an indefinite mechanism - the ventricles eventually lose function due to reduced interactions between myocardial cells due to increased distance between them [28].
Compensatory mechanism through activation of the neurohumoral system:
Sympathetic nervous system: Sympathetic activation of the adrenergic system leads to vasoconstriction, increasing resistance to blood flow and helping to maintain arterial pressure in the early stages of heart failure when cardiac output is reduced. The increase in heart rate and myocardial contractility due to sympathetic activation helps to regulate cardiac output closer to normal. However, long-term sympathetic stimulation will also lead to a decrease in beta-receptor density in myocardial fibers and a gradual decrease in response to catecholamines [5].
Renin-angiotensin-aldosterone system (RAAS): Increased activity of the sympathetic system also activates the RAAS. Renin released from the kidney increases the formation of angiotensin I from angiotensinogen and is converted to angiotensin II by the action of angiotensin-converting enzyme (ACE). Angiotensin II causes systemic vasoconstriction and acts on the adrenal cortex to produce aldosterone, leading to sodium and water retention. In addition, aldosterone also causes myocardial and vascular fibrosis. Sympathetic stimulation also releases antidiuretic hormone (ADH), which causes water retention and contributes to hyponatremia [28].
Arginine-vasopressin system: in late-stage heart failure, the hypothalamus and pituitary are stimulated to secrete arginine-vasopressin, which increases the peripheral vasoconstrictor effect of angiotensin II, while increasing water reabsorption in the renal tubules. All three of these vasoconstrictor systems aim to maintain cardiac output, but over time they increase preload and afterload, increase water and salt retention, increase myocardial work and oxygen consumption, creating a vicious cycle that worsens heart failure [5].
Natriuretic peptides: Including A- and B-type natriuretic peptides (ANP and BNP) secreted by myocardial cells in response to atrial and ventricular stretch/distension; C-type natriuretic peptides secreted by the endothelium and kidney. Natriuretic peptides, mainly BNP, lead to increased sodium excretion and vasodilation, especially in the early stages of heart failure. BNP also has anti-myocardial remodeling properties. The biological response of BNP is mediated by natriuretic peptide receptors (NPR). Human